Questions
- What is the impact of supervised drug consumption services (SCS)?
Key take-home messages
- Three systematic reviews (1–3) and one scoping review (4) published in peer-reviewed journals have found evidence that SCS can provide individual- and community-level benefits. Some of the individual-level benefits include reducing infections related to drug use, reducing the risk of non-fatal overdose, and facilitating access to health services (4). Community-level benefits include reduction in public disorder (e.g. less use of drugs in public spaces and less public disposal of syringes) and a decrease in the use of other public services (e.g. ambulance transport to hospital) (4). SCS have not been found to be associated with an increase in drug-related crime (4).
- Peer-reviewed primary studies published in recent years continue to demonstrate that SCS meet their overall objectives such as: management of drug overdose and decreased mortality (5), enhancement of safer injecting practices (6), receipt of services by the most high-risk, marginalized people who use drugs (7), less improper syringe disposal in public places (8), decreased public drug use (9), increased uptake of addiction treatment and other healthcare and social services (10), and prevention of transmission of blood-borne diseases (11–13), without increases in crime (14), drug use, or overdose rates (9).
- Evaluations of SCS have mostly relied upon ecological, modelling, cross-sectional, and cohort study designs to draw conclusions about the impact of SCS (2, 15, 16). Although these evaluation methodologies have been established in the literature and are appropriate given the context, further research could involve systematic inclusion of a control group who are eligible but do not access SCS (15). While some study cohorts include individuals who use SCS as well as those who do not (17), the body of evidence for SCS in general could be strengthened by inclusion of randomized controlled trials (1, 4, 18) and by a broader range of settings and jurisdictions to enhance generalizability (1, 18).
The issue and why it’s important
Supervised drug consumption sites or services (SCS) refer to spaces where individuals can use pre-obtained illicit substances in the presence of trained health professionals (19, 20). A model of care based on harm reduction, SCS are an evidence-based intervention (21–24) aiming to reduce the health and social harms associated with addiction or substance use by offering a range of low-barrier services to people who use drugs (25).
The primary goals of SCS are consistent across sites worldwide (26), but their design and operation can differ based on the local needs and context in which they operate (27). In Canada, services and supports provided by SCS typically include:
- a safe and hygienic environment to inject, snort, swallow or—less commonly—smoke drugs
- sterile drug use equipment and safe disposal of equipment after use
- supervision and safer drug use education
- staff to monitor for signs of overdose and provide emergency overdose intervention
- naloxone distribution and training
- referrals and linkage to drug treatment and other health and social services (e.g. housing services, primary healthcare, mental health services)
- basic medical care, such as wound care (27).
Some SCS in Canada also offer testing for HIV, hepatitis C (HCV), sexually transmitted infections (STIs), and drug checking to determine the contents of a drug sample (27). To legally operate SCS for medical purposes in Canada, a valid exemption under section 56.1 of the Controlled Drugs and Substances Act (CDSA) is necessary (28, 29). As of December 2023, 39 sites across Canada are offering supervised consumption to the public (28). It is estimated that between 2017 and June 2023, 4.3 million visits occurred at Canadian SCS among at least 361,000 unique clients (30). Figure 1 outlines SCS usage statistics in Canada (30).
| Figure 1. Usage of SCS in Canada, 2017–June 2023 (29) • SCS were visited 4.3 million times by at least 361,000 unique individuals • Some SCS accommodated up to 400 visits per day • 34% of SCS clients were between the ages of 30-39 years old • 49,000 overdoses and drug-related emergencies were attended to • No reported fatalities occurred on-site • Approximately 70% of the substances consumed at SCS in Canada were opioids, primarily fentanyl and hydromorphone (Dilaudid) • The use of the stimulant drug methamphetamine is also prevalent among clients of SCS • Around 257,000 SCS clients received referrals to substance use treatment and other health services (e.g. medical care, mental health support, housing services) |
Health Canada lists all 39 sites that have a valid exemption under section 56.1 of the CDSA on their website, and includes a description of the authorized services available at each location (28). This can vary: some sites support multiple routes of drug consumption including inhalation, injection, intranasal, and oral (28), while others focus on a smaller range of core services such as injection drug use and drug checking (28).
Sites that offer injection drug use as the only route of administration are often called supervised injection sites (SIS) or supervised injection facilities (SIF). While much of the existing research on SCS is focused specifically on injection drug use (31, 32), there appears to be a growing focus on SCS in Canada that would support drug consumption through other routes of administration, especially inhalation (33–35). While supported by research in the peer-reviewed literature (21–24, 36, 37) and by the Government of Canada (38), SCS continue to be a topic of controversy (25, 36, 39). This review briefly describes the methodology used to assess the impact of SCS and explores the outcomes of this intervention as described in peer-reviewed and grey literature. In addition to the aforementioned terms such as SIS and SIF, several other terms are used to describe SCS in the literature (40), including, but not limited to, supervised consumption facilities (SCF), drug consumption rooms (DCR), or medically supervised injecting rooms (MSIR). When discussing individual studies, the term used in the study will be applied in this review; when discussing supervised drug use sites in general, the term SCS will be used.
What we found
Methodology to assess supervised consumption services
Numerous primary studies and systematic reviews have been published evaluating SCS in different jurisdictions. These studies have used a variety of indicators to assess the impact of SCS (15). Table 1 (below), created by the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) in 2010, outlines the Aims that SCS generally set out to accomplish, the Outcome Objectives to be achieved by the SCS, and the measurable Indicators used to determine if the outcomes are being achieved (26).
Table 1. Aims, outcome objectives, and indicators of drug consumption rooms (25)
| Aims | Outcomes | Objectives |
| 1. Provide an environment for safer drug use | a) Reach and be accepted by target groups b) Gain acceptability c) Establish conditions for safe, hygienic use | Client profiles, service use patterns, client satisfaction Responses of local residents, businesses, police, politicians Various process indicators |
| 2. Improve health status of target group | a) Improve risk-related behaviours b) Reduce morbidity c) Reduce mortality d) Improve access to healthcare and drug treatment | Street drug use, risk awareness, injection hygiene, borrowing/lending Injection injuries, infectious disease transmission Overdose outcomes Treatment referral/uptake |
| 3. Reduce public disorder | a) Reduce public drug use b) Improve public perceptions c) No increases in local drug-related crime | Self-reported rates of public injecting, ethnographic observations of the burden of public injecting Perceived nuisance, discarded syringes Crime statistics |
The indicators provided in Table 1 can be corroborated with a 2019 systematic review by Belackova et al. (2019) which focused on describing and assessing the methodologies used to evaluate DCR/SIF (15). Belackova et al. (2019) created a list of eight outcome measures for individuals and the community that have been used to evaluate SCS (15). These include:
- Attracting high-risk, marginalized users
- Management of overdose and decreased mortality
- Enhancement of safe injecting practices
- Decreased public drug use and improved public amenity
- Increased uptake of treatment and other healthcare and social services
- Prevention of transmission of blood-borne diseases and the associated economic benefits from it
- No increase in crime
- No increase in drug use or related risks
While there is an abundance of literature that examines the impact and effectiveness of SCS, it appears that few studies utilize an experimental design (2, 24, 26, 41, 42). One reason for this is due to some practical and ethical problems that may be associated with experimental study designs (15). For example, imposing enrollment in a low-threshold, harm-reduction program on a random sample of people who use drugs while at the same time depriving others from the program is both impractical and unethical; this is especially true for SCS, where there is good evidence for overdose intervention and other positive outcomes (15). Furthermore, the abundance of observational studies “…reflects the reality that SIFs are first and foremost community responses to crises; structuring ideal research conditions is, rightly, not their priority” (1). While experimental study designs (e.g. randomized controlled trials) are typically considered the gold standard in measuring intervention effectiveness, given the ethical issues and impracticality of conducting randomized controlled trials in the context of SCS, several studies deem that the published literature that has used non-experimental methods to assess SCS is sufficient (2, 15, 26, 41).
Peer-reviewed systematic and scoping reviews assessing supervised consumption services
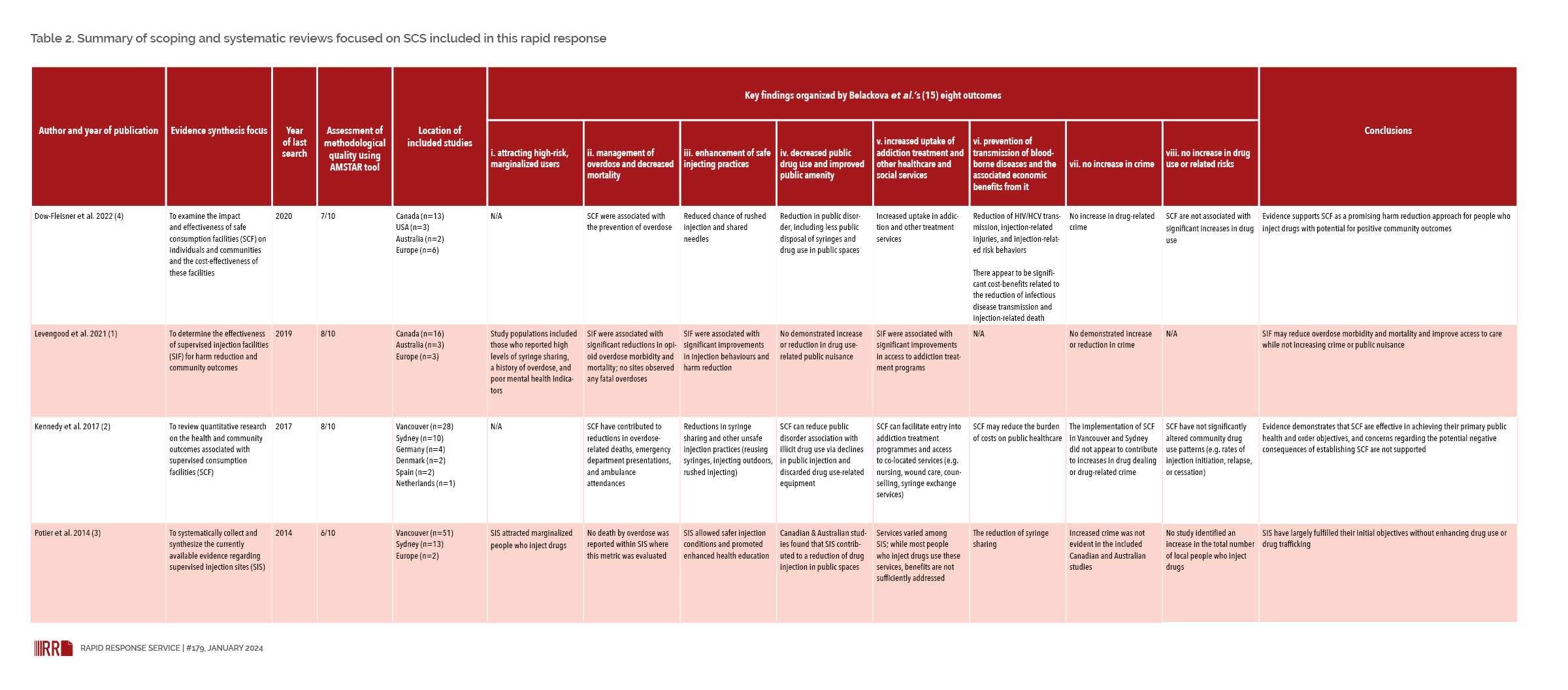
We identified three systematic reviews (1–3) and one scoping review (4), published in peer-reviewed journals within the last ten years, that focused on evaluating SCS. Table 2 describes the features of these four reviews, provides results of assessment of their methodological quality (43), and organizes the findings according to Belackova et al.’s eight outcomes. Not included in Table 1 is a meta-analysis on impacts of SCS on drug-related harms by May et al. (2018) (44), published in 2018 and subsequently retracted, due to “methodological weaknesses linked to the pooling of diverse outcomes into a single composite measure” (45).
The primary model of SCS in all four reviews were fixed locations within a community (1–4). Two reviews focused on sites offering supervised injection services (1, 3) while the other two reviews also included sites offering services via other routes of consumption; the majority of included studies were based on supervised injection services (2, 4). Across all four reviews, most studies were based in Vancouver, followed by Australia (1–4). Few studies from the U.S. and Europe were identified (1–4).
All four reviews concluded that supervised consumption sites have positive outcomes for people who use drugs (1–4). This included a decrease in overdose-related deaths, improvements in injection-related behaviours, increased uptake of services (addiction counselling, wound care, etc.), and no increase in drug use (1–4). Several outcomes at the community level were also identified: rates of crime did not increase, and no significant increases in drug use were observed (1–4). Additionally, the reviews concluded that concerns regarding potential negative consequences of SCS are largely unfounded (1–4). In addition to these four reviews, other systematic reviews have discussed SCS in the context of programming for people who use drugs. One review found that among people experiencing homelessness, the provision of these services decreased the number of fatal overdoses, high-risk behaviours, and improved access to care (46). Another review concluded that supervised injection facilities provided an important health service to prevent infectious diseases among people who inject drugs (47).
Table 2. Summary of scoping and systematic reviews focused on SCS included in this rapid response
Click to expand or download table as PDF
Grey literature reports assessing supervised consumption services
Reports from organizations
There have been several reports on SCS published online. In addition to the systematic review on DCR/SIF methodology discussed above (15), Belackova et al. (2017) wrote a review for the United Medically Supervised Injecting Centre in Sydney, Australia, collating all the literature relevant to DCR/SIF (24). Numerous studies found that DCR/SIF engaged high-risk users, enhanced safer injecting practices, managed overdoses, decreased rates of overdoses, yielded cost-savings, and did not increase drug use or crime (24).
Two online reports did mathematical modelling to estimate the potential impacts of opening hypothetical SCS. The Lankenau Institute for Medical Research in Pennsylvania estimated that between 1–18 cases of HIV and 15–213 infections of HCV could be averted annually for a hypothetical SCF located in Philadelphia (48). Additionally, drug overdoses could potentially be reduced by a range of 24 to 76 each year (48). A 2021 report published by the Institute for Clinical and Economic Review concluded that operating an SIF would result in fewer lives lost, reduce costs associated with overdoses, and reduce costs overall when compared with operating a standalone syringe service program (49).
The RAND Corporation, a U.S. research institute, published a review in 2018 that assessed the evidence of SCS (50). Authors summarized their findings into three key insights, listed below as direct quotes:
- Overall, the scientific evidence on the effectiveness of SCSs is limited in quality and number of locations evaluated (50).
- Estimating the overall effect of SCSs on fatal and non-fatal overdoses is difficult (50).
- For drug consumption that is supervised, SCSs reduce the risk of disease transmission and other harms associated with unhygienic drug use practices; however, there is uncertainty about the size of the overall effect (50).
Government reports
The Government of Alberta published the results of a review on SCS in 2020 and found that, with the exception of Edmonton, crime (measured by police calls) had increased in the immediate vicinity when compared to areas outside of the immediate vicinity (51). Additionally, the report states that a variety of issues were raised at public consultations, including “…increases in needle debris to increases in crime, and increases in overall social disorder since the sites opened” (68). A response to this report was published in 2021 in a peer-reviewed journal, and stated that due to methodological limitations of the government report, the measured change in crime was poorly assessed (25). The Government of Victoria in Australia published a report in February of 2023 evaluating the Medically Supervised Injecting Room (MSIR) in the North Richmond neighbourhood of Melbourne (52). The report found that the MSIR reduced deaths and overdose related harm, provided access to general health and social assistance, reduced hospital and ambulances attendances, and reduced the spread of blood-borne viruses (based on testing, onsite treatment, and linkage to care) (52). However, based on community feedback, the report did identify that publicly discarded needles and syringes remain a challenge, and that local residents sometimes felt unsafe due to individuals congregating outside of the MSIR (52).
Recently published primary studies assessing supervised consumption services
Evidence evaluating the impact of SCS continues to be published in the peer-reviewed literature. It should be mentioned that in our Rapid Response from 2021 on SCS, we included a section (Table 1 in Rapid Response #157) that lists all of the outcomes in Belackova et al. (2019) and cites a selection of studies (published between 2005–2021) that report on these outcomes (53).
Several more recently published studies (2021–2023) that were not included in the above-discussed systematic reviews have found that SCS:
- can engage socially vulnerable people who use drugs (7)
- are associated with a decrease in fentanyl-related overdose deaths (5)
- may reduce receptive syringe sharing and injecting in isolated locations (6)
- reduce the rate of syringes disposed in public places (e.g. street, sidewalk, park) (8)
- decrease public drug use (9)
- increase participation in addiction treatment (10)
- successfully test and provide HCV treatment (11)
- provide cost-savings when overdoses are managed at SCS (13)
- can reduce drug-related incidents (e.g. crimes involving the dealing or possession of drugs) in the vicinity of the SCS (14)
- can mitigate the risk of drug overdose through trained staff (9).
None of these recent studies were captured in the peer-reviewed systematic or scoping reviews discussed above (1–4, 15), nor were they included in our 2021 Rapid Response on SCS (53). Thus, it appears that recently published studies continue to demonstrate the positive impacts that SCS may have on individuals and within communities. It should also be noted that similar to the primary studies included in the aforementioned systematic reviews, almost all of the study designs utilized were observational; none used an experimental study design except two studies that used a quasi-experimental design (14, 54).
Factors that may impact local applicability
Globally, supervised consumption sites and services are offered in a limited number of countries (55). As noted by Caulkins et al. (2019), a large amount of literature examining SCS comes from Australia and Vancouver (42). However, we did identify and include more recent studies from the U.S. that examined one unsanctioned SCS at an undisclosed location (6, 8, 14) and one study that presented preliminary findings from two SCS in New York City (9). Furthermore, the majority of studies we identified examined injection drug use; this reflects the broader literature base, which has limited evidence on SCS for people that use drugs orally, intranasally, or by inhalation (31).
Additionally, SCS vary in terms of what services are offered, the number of individuals that can be accommodated, hours of operation, staff qualifications, and the settings in which they operate; thus, findings may not be generalizable to all SCS (42). Finally, as discussed in this review, there is a lack of studies evaluating SCS that use experimental designs (2, 24, 26, 41, 42). Thus, findings discussed in this review are associations based on observational research, and not indicative of definitive cause-and-effect relationships.
What we did
We searched Medline (including Ovid MEDLINE and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations) and PsycInfo using terms (supervised drug consumption* or drug consumption room*or drug consumption facilit* or Overdose Prevention Site* or supervised consumption or harm reduction cen* or Consumption adj3 Service* or Supervised Injection or overdose prevention cen* or safe* injection or safe* consumption) in titles or abstracts. Searches were conducted on August 28, 2023 and results limited to articles published from 2015 to present in English. Only studies conducted in high-income countries were included. Reference lists of identified articles were also searched. Google (grey literature) searches using different combinations of these terms were also conducted. The searches yielded 1,061 references from which 55 were included.
Reference list
- Levengood TW, Yoon GH, Davoust MJ, Ogden SN, Marshall BD, Cahill SR, et al. Supervised injection facilities as harm reduction: A systematic review. American Journal of Preventive Medicine. 2021;61(5):738–49.
- Kennedy MC, Karamouzian M, Kerr T. Public health and public order outcomes associated with supervised drug consumption facilities: A systematic review. Current HIV/AIDS Reports. 2017;14(5):161–83.
- Potier C, Laprévote V, Dubois-Arber F, Cottencin O, Rolland B. Supervised injection services: What has been demonstrated? A systematic literature review. Drug and Alcohol Dependence. 2014;145:48–68.
- Dow-Fleisner SJ, Lomness A, Woolgar L. Impact of safe consumption facilities on individual and community outcomes: A scoping review of the past decade of research. Emerging Trends in Drugs, Addictions, and Health. 2022;2(100046).
- Marshall T, Abba-Aji A, Tanguay R, Greenshaw AJ. The impact of supervised consumption services on fentanyl-related deaths: Lessons learned from Alberta’s provincial data. Canadian Journal of Psychiatry. 2021;66(12):1096–8.
- Suen LW, Davidson PJ, Browne EN, Lambdin BH, Wenger LD, Kral AH. Effect of an unsanctioned safe consumption site in the United States on syringe sharing, rushed injections, and isolated injection drug use: A longitudinal cohort analysis. Journal of Acquired Immune Deficiency Syndromes. 2022;89(2):172–7.
- Van Den Boom W, del Mar Quiroga M, Fetene DM, Agius PA, Higgs PG, Maher L, et al. The Melbourne safe injecting room attracted people most in need of its service. American Journal of Preventive Medicine. 2021;61(2):217–24.
- Kral AH, Lambdin BH, Wenger LD, Browne EN, Suen LW, Davidson PJ. Improved syringe disposal practices associated with unsanctioned safe consumption site use: A cohort study of people who inject drugs in the United States. Drug & Alcohol Dependence. 2021;229(Pt A):109075.
- Harocopos A, Gibson BE, Saha N, McRae MT, See K, Rivera S, et al. First 2 months of operation at first publicly recognized overdose prevention centers in US. JAMA Network Open. 2022;5(7):e2222149.
- Kennedy MC, Hayashi K, Milloy M, Compton M, Kerr T. Health impacts of a scale-up of supervised injection services in a Canadian setting: An interrupted time series analysis. Addiction. 2022;117(4):986–97.
- Lettner B, Mason K, Greenwald ZR, Broad J, Mandel E, Feld JJ, et al. Rapid hepatitis C virus point-of-care RNA testing and treatment at an integrated supervised consumption service in Toronto, Canada: A prospective, observational cohort study. Lancet Regional Health Americas. 2023;22:100490.
- Greenwald ZR, Bouck Z, McLean E, Mason K, Lettner B, Broad J, et al. Integrated supervised consumption services and hepatitis C testing and treatment among people who inject drugs in Toronto, Canada: A cross-sectional analysis. Journal of Viral Hepatitis. 2023;30(2):160–71.
- Khair S, Eastwood CA, Lu M, Jackson J. Supervised consumption site enables cost savings by avoiding emergency services: A cost analysis study. Harm Reduction Journal. 2022;19(1):32.
- Davidson PJ, Lambdin BH, Browne EN, Wenger LD, Kral AH. Impact of an unsanctioned safe consumption site on criminal activity, 2010–2019. Drug & Alcohol Dependence. 2021;220:108521.
- Belackova V, Salmon AM, Day CA, Ritter A, Shanahan M, Hedrich D, et al. Drug consumption rooms: A systematic review of evaluation methodologies. Drug & Alcohol Review. 2019;38(4):406–22.
- Concato J, Shah N, Horwitz RI. Randomized, controlled trials, observational studies, and the hierarchy of research designs. New England Journal of Medicine. 2000;342(25):1887–92.
- Scheim AI, Sniderman R, Wang R, Bouck Z, McLean E, Mason K, et al. The Ontario integrated supervised injection services cohort study of people who inject drugs in Toronto, Canada (OiSIS-Toronto): Cohort profile. Journal of Urban Health. 2021;98(4):538–50.
- May T, Holloway K, Bennett T. The need to broaden and strengthen the evidence base for supervised consumption sites. Addiction. 2019;114(12):2117–8.
- City of Toronto. Supervised consumption services. 2023. Available from: https://www.toronto.ca/community-people/health-wellness-care/health-programs-advice/supervised-injection-services/ Accessed September 21, 2023.
- Rubin R, Suran M. Supervised consumption sites—A tool for reducing risk of overdose deaths and infectious diseases in people who use illicit drugs. Journal of the American Medical Association. 2022;327(16):1532–4.
- European Monitoring Centre for Drugs and Drug Addiction. Drug consumption rooms: An overview of provision and evidence. 2018. Available from: https://www.emcdda.europa.eu/publications/pods/drug-consumption-rooms_en Accessed September 30, 2023.
- Abram MD, Seabra P, Searby A. Supervised drug consumption sites: A health-based approach or enabling drug use? Journal of Clinical Nursing. 2023;32(7–8):e6–e8.
- Yoon GH, Levengood TW, Davoust MJ, Ogden SN, Kral AH, Cahill SR, et al. Implementation and sustainability of safe consumption sites: A qualitative systematic review and thematic synthesis. Harm Reduction Journal. 2022;19(1):73.
- Belackova VS, Salmon AM. Supervised injecting facilities & drug consumption rooms. 2017. Available from: https://www.uniting.org/content/dam/uniting/documents/community-impact/uniting-msic/overview-of-international-literature.pdf Accessed January 4, 2024.
- Livingston JD. Supervised consumption sites and crime: Scrutinizing the methodological weaknesses and aberrant results of a government report in Alberta, Canada. Harm Reduction Journal. 2021;18(1):4.
- European Monitoring Centre for Drugs and Drug Addiction. Harm reduction: Evidence, impacts and challenges. 2010. Available from: https://www.emcdda.europa.eu/publications/monographs/harm-reduction_en Accessed September 28, 2023.
- Arkell C. Harm reduction in action: Supervised consumption services and overdose prevention sites. 2018. Available from: https://www.catie.ca/prevention-in-focus/harm-reduction-in-action-supervised-consumption-services-and-overdose Accessed September 21, 2023.
- Health Canada. Supervised consumption sites: Status of applications. 2024. Available from: https://www.canada.ca/en/health-canada/services/substance-use/supervised-consumption-sites/status-application.html Accessed January 4, 2024.
- Health Canada. Application form: Section 56.1 Exemption for Medical Purposes under the Controlled Drugs and Substances Act for activities at a supervised consumption site. 2018. Available from: https://www.canada.ca/content/dam/hc-sc/documents/services/substance-abuse/supervised-consumption-sites/apply/how-to-apply.pdf Accessed January 3, 2024.
- Government of Canada. Data blog: Supervised consumption sites. Available from: https://health-infobase.canada.ca/datalab/supervised-consumption-sites-blog.html Accessed October 4, 2023.
- Speed KA, Gehring ND, Launier K, O’Brien D, Campbell S, Hyshka E. To what extent do supervised drug consumption services incorporate non-injection routes of administration? A systematic scoping review documenting existing facilities. Harm Reduction Journal. 2020;17(1):72.
- Gehring ND, Speed KA, Launier K, O’Brien D, Campbell S, Hyshka E. The state of science on including inhalation within supervised consumption services: A scoping review of academic and grey literature. International Journal of Drug Policy. 2022;102:103589.
- Bourque S, Pijl EM, Mason E, Manning J, Motz T. Supervised inhalation is an important part of supervised consumption services. Canadian Journal of Public Health Revue Canadienne de Sante Publique. 2019;110(2):210–5.
- Casey House. Casey House opens first indoor supervised inhalation space for substance use. 2022. Available from: https://caseyhouse.ca/commentary/casey-house-opens-first-indoor-supervised-inhalation-space-for-substance-use/ Accessed September 30, 2023.
- Partridge K. Supervised inhalation sites take surprising forms in B.C. amid challenges setting them up. 2022. Available from: https://www.cbc.ca/news/canada/british-columbia/smoking-substances-solutions-toxic-drug-crisis-1.6823856 Accessed September 30, 2023.
- Kennedy MC, Karamouzian M, Marshall BDL. The North American opioid crisis: How effective are supervised consumption sites? Lancet. 2022;400(10361):1403–4.
- Ng J, Sutherland C, Kolber MR. Does evidence support supervised injection sites? Canadian Family Physician. 2017;63(11):866.
- Government of Canada. Supervised consumption sites. Dashboard. Last updated: 2023-11-15. Available from: https://health-infobase.canada.ca/supervised-consumption-sites/ Accessed December 19, 2023.
- Casey L. New supervised consumption sites in Ontario on hold until review complete. 2023. Available from: https://www.cp24.com/news/new-supervised-consumption-sites-in-ontario-on-hold-until-review-complete-1.6590507 Accessed October 2023.
- Moledina A, Magwood O, Agbata E, Hung JH, Saad A, Thavorn K, et al. A comprehensive review of prioritised interventions to improve the health and wellbeing of persons with lived experience of homelessness. Campbell Systematic Reviews. 2021;17(2):e1154.
- Maher L, Salmon A. Supervised injecting facilities: How much evidence is enough? Drug and Alcohol Review. 2007;26(4):351–3.
- Caulkins JP, Pardo B, Kilmer B. Supervised consumption sites: A nuanced assessment of the causal evidence. Addiction. 2019;114(12):2109–15.
- Shea BJ, Grimshaw JM, Wells GA, Boers M, Andersson N, Hamel C, et al. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Medical Research Methodology. 2007;7:1–7.
- May T, Bennett T, Holloway K. RETRACTED: The impact of medically supervised injection centres on drug-related harms: A meta-analysis. International Journal of Drug Policy. 2018;59:98–107.
- May T, Bennett T, Holloway K. RETRACTED: The impact of medically supervised injection centres on drug-related harms: A meta-analysis. International Journal of Drug Policy 2018;9:98–107.
- Magwood O, Salvalaggio G, Beder M, Kendall C, Kpade V, Daghmach W, et al. The effectiveness of substance use interventions for homeless and vulnerably housed persons: A systematic review of systematic reviews on supervised consumption facilities, managed alcohol programs, and pharmacological agents for opioid use disorder. PLoS ONE. 2020;15(1):e0227298.
- Bouzanis K, Joshi S, Lokker C, Pavalagantharajah S, Qiu Y, Sidhu H, et al. Health programmes and services addressing the prevention and management of infectious diseases in people who inject drugs in Canada: A systematic integrative review. BMJ Open. 2021;11(9):e047511
- Larson S, Padron N, Mason J, Bogaczyk T. Supervised consumption facilities—Review of the evidence. 2017. Available from: https://dbhids.org/wp-content/uploads/2018/01/OTF_LarsonS_PHLReportOnSCF_Dec2017.pdf Accessed October 3, 2023.
- Armbrecht E, Guzauskas G, Hansen R, Pandey R, Fazioli K, Chapman R, et al. Supervised injection facilities and other supervised consumption sites: Effectiveness and value. Final evidence report. 2021. Available from: https://icer.org/wp-content/uploads/2020/10/ICER_SIF_Final-Evidence-Report_010821.pdf Accessed October 4, 2023.
- Pardo B, Caulkins J, Kilmer B. Assessing the evidence on supervised drug consumption sites. 2018. Available from: https://www.rand.org/pubs/working_papers/WR1261.html Accessed October 4, 2023.
- Government of Alberta. Impact: A socio-economic review of supervised consumption sites in Alberta. 2020. Available from: https://open.alberta.ca/publications/9781460147054 Accessed October 4, 2023.
- Government of Australia. Final report: Key findings and recommendations. 2023. Available from: https://content.health.vic.gov.au/sites/default/files/2023-03/review-of-the-msir-final-report-february-2023.pdf Accessed October 4, 2023
- The Ontario HIV Treatment Network. A review of structural, process, and outcome measures for supervised consumption services. 2020. Available from: https://www.ohtn.on.ca/wp-content/uploads/2021/07/RR157_SCS-measures.pdf Accessed October 4, 2023.
- Kennedy MC, Hayashi K, Milloy MJ, Compton M, Kerr T. Health impacts of a scale-up of supervised injection services in a Canadian setting: An interrupted time series analysis. Addiction. 2022;117(4):986–97.
- Colledge-Frisby S, Ottaviano S, Webb P, Grebely J, Wheeler A, Cunningham EB, et al. Global coverage of interventions to prevent and manage drug-related harms among people who inject drugs: A systematic review. The Lancet Global Health. 2023;11(5):e673–e83.
Suggested citation
Rapid Response Service. The impact of supervised drug consumption services (SCS). Toronto, ON: The Ontario HIV Treatment Network; January 2024.
Prepared by
Danielle Giliauskas and David Gogolishvili
Illustration credit
Rachel Chung