1
With respect, the OHTN acknowledges that in our collaborations across Ontario, we work in the traditional territories of Cree, Anishnabe, Haudenosaunee, Ojibway/Chippewa, Attawandaron, Wendat and Oneida peoples. Forty-six treaties and agreements cover Ontario. We are all treaty people responsible for reconciliation and justice.
Can the 4th decade of HIV/AIDS be the last?
Ontario and the rest of the developed world are at a tipping point in our efforts to stop HIV.
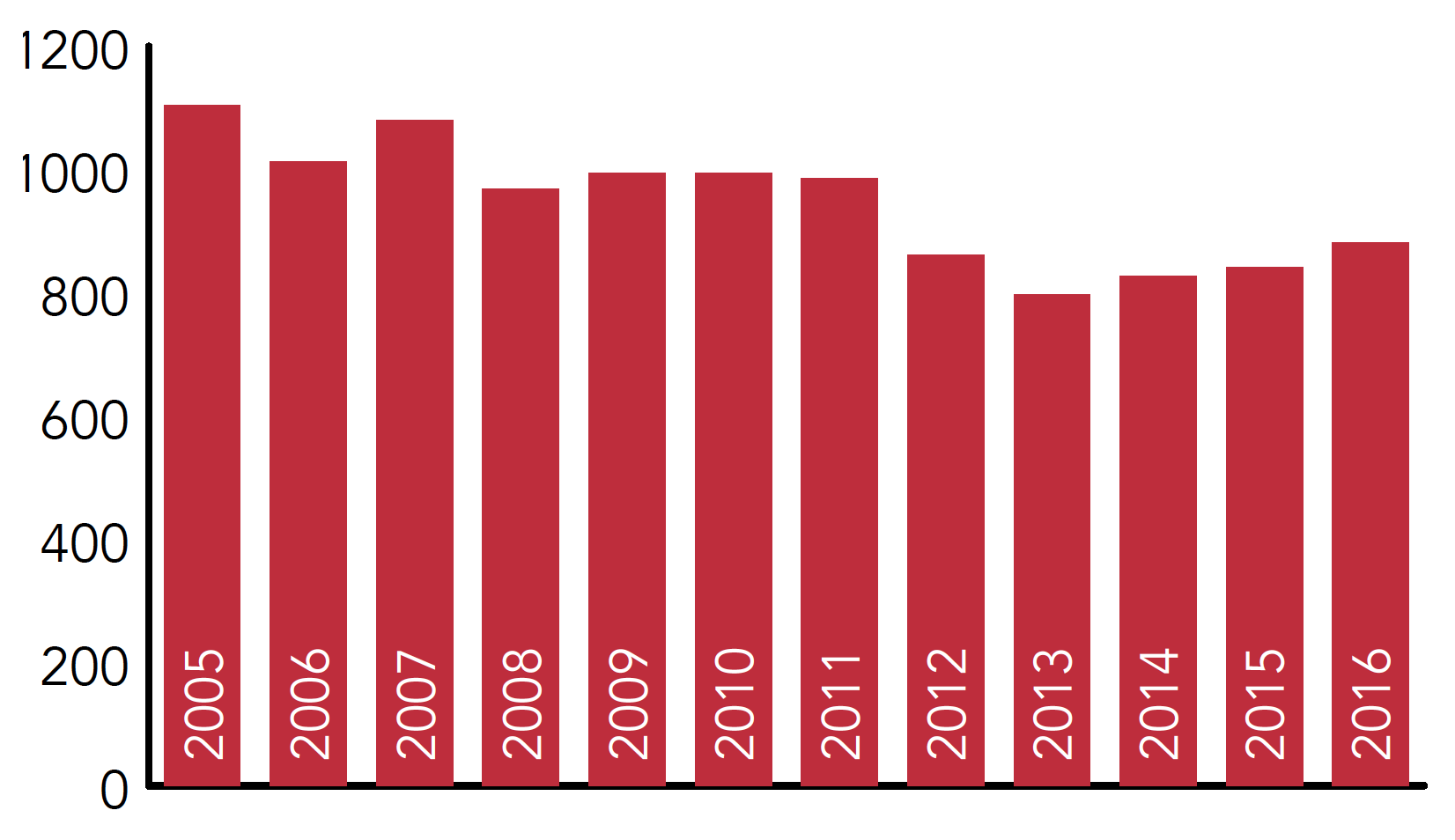
Over the past 30+ years, we have made incredible progress. We now have highly effective treatments and new approaches to prevention. We are seeing fewer new HIV diagnoses each year than five years ago and fewer AIDS deaths.
We know that early and ongoing antiretroviral treatment improves the health of people living with HIV and reduces the risk of transmission.
New HIV diagnoses, Ontario, 2005-2016
We now have medications—pre-exposure prophylaxis (PrEP) and post-exposure prophylaxis (PEP)—that can protect people at high risk.
We also have a clearer understanding of how the broader social determinants of health—poverty, housing instability, food insecurity, mental health issues, addictions, violence, abuse, stigma, and social and structural inequities—put people at risk and threaten the health of people living with HIV.
Over the next 10 years, we can use the knowledge, treatments and prevention tools we already have to implement innovations that will allow Ontario to reach the endgame.
Can the fourth decade of HIV/AIDS be the last? Or will be lose our sense of urgency and become complacent because HIV is less of a threat and the job is almost done?
Someone diagnosed today with HIV faces a very different trajectory than someone diagnosed in the 1980s. In 2017, people with HIV who are diagnosed early, engaged in care and receive treatment to suppress the virus—as well as high quality care for other health issues—can enjoy a life expectancy approaching that of the general population. The prognosis is not as hopeful for people with HIV who struggle with the basics of life and/or have other serious health and social issues, such as mental health issues, an addiction or unstable housing.
2
“Twenty years ago, the Ontario government brought together people living with HIV, community-based workers, health care providers and researchers. Together, we invented the Ontario HIV Treatment Network to improve the delivery of new treatments to people across Ontario. Today, our concept of treatment has expanded to include medical and mental health care, social support, prevention and quality of life for people living with HIV. Working proudly and passionately, Ontario has built services that provide health, support and justice to people living with and at risk of HIV. I am excited by the OHTN’s new strategic plan to bring our strengths together to create an integrated and supportive network of services that can make this the last decade of HIV in Ontario. ”Murray Jose-Boerbridge, Co-Chair, First OHTN Board 1998-2000
Time for us to up our game
In chess, the most important part of the game is the endgame. It is at this stage, where there are fewer pieces on the board, that tactical thinking is key. People can have an overwhelming advantage in chess—just as we do right now with HIV—but lose because of poor tactics in the endgame. To make the fourth decade the last, the Ontario HIV Treatment Network (OHTN must make the kind of strategic moves that will ensure we reach and win the endgame.
The next five to ten years cannot be business as usual. The OHTN must focus our efforts and resources where they can have the greatest impact. We must fundamentally re-orient our organization, shifting our focus and taking a more proactive, coordinated approach to driving change based on data and evidence.
Who we are
The OHTN is a nonprofit, stakeholder-driven organization funded by the AIDS Bureau of the Ministry of Health and Long-Term Care to gather and analyze data, implement and assess innovation, and work with care providers and communities to make a collective impact – changing and improving the way we work together.
Our vision
Communities thriving now and beyond HIV.
HIV affects individuals and their communities. In Ontario, the virus has had a particularly devastating effect on gay men as well as men and women who inject drugs and those who are members of Ontario’s African Caribbean and Black (ACB) communities and Indigenous communities. Through our work, we strive to support these communities’ efforts to live and thrive with HIV, and to see beyond HIV so they can prosper in all aspects of their lives.
Our mission
To improve the health and lives of people with and at risk of HIV by using data and evidence to drive change.
The OHTN works to influence decision-making at all levels—personal, clinical, organizational and policy—by working collaboratively with our partners to gather and analyze data, implement innovation and support the integration and best use of the knowledge we gather.
The current landscape
Over the past 30+ years, the landscape for the HIV sector and for the OHTN’s work has evolved dramatically—driven by new knowledge and tools, changes in policy and broader system changes. In 2017, we see both new opportunities to help us reach and win the endgame as well as challenges that may make it harder to achieve our goals.
UN AIDS Targets
Opportunities
- The UNAIDS targets focus health systems on measurable goals that will improve the health of people with HIV and reduce the risk of new infections.
- A clear understanding of the prevention, engagement and care cascades in Ontario, with tools and systems in place to measure outcomes for the populations effected by HIV.
- A bigger prevention toolbox and a new focus on biomedical prevention including treatment as prevention, PrEP and non-occupational post-exposure prophylaxis (nPEP).
- A system-wide push for patient-centred care, more focus on quality and accountability and growing efforts to tackle the social and structural drivers of HIV such as stigma, a history of violence or trauma, mental health problems, addictions, poverty and unstable housing.
Challenges
- The capacity of the HIV sector to adopt/adapt evidence-based practices. Ontario’s HIV sector consists of many small community-based organizations and programs and small specialized HIV clinics and primary care practices. Over the past few years, HIV clinics have faced budget cuts and have lost staff, hours or both. Many AIDS service organizations (ASOs) have lost federal funding.
- A number of clinical and community leaders have retired or died and more will follow over the next five to ten years. The long-time leaders are being replaced by people who work only a few years in the field and then move on. Creating a rapid learning community in this changing environment is challenging.
- As HIV treatments have improved, clinicians now need more information related to managing HIV co-morbidities and people aging with HIV. The sector also needs information on the factors driving new infections.
Our criteria for investment and involvement
The HIV sector is taking a three-pronged approach to stopping HIV:
- Change the HIV prevention, engagement and care cascade – intervening at each stage of the cascade to help people maintain and improve their health.
- Target resources to the people and populations most affected by HIV.
- Take a systems approach, integrating HIV services with other health and social services that people affected by HIV need.
As part of our commitment to focus our efforts and ensure accountability for our use of public resources, the OHTN will invest only in data analytics, implementation projects, rapid learning, and ‘backbone’ programs and initiatives that are:
3
“Large-scale social change requires broad cross-sector coordination, yet the social sector remains focused on the isolated intervention of individual organizations.”Collective Impact, John Kania and Mark Kramer, 2011
The OHTN’s strategic directions to 2026
The OHTN will pursue four key strategic directions:
- Gather and analyze data on the HIV epidemic and HIV programs and services.
- Implement and assess care and service innovations.
- Support the use of the best available data and evidence.
- Help create the backbone for collective impact (i.e. coordination/collaboration) in the HIV sector.
Gather and analyze data on the HIV epidemic and HIV programs and services
The programs
The OHTN currently has four distinct data analytics programs:
- The Ontario HIV Epidemiology and Surveillance Initiative (OHESI)—a collaboration among the OHTN, the AIDS Bureau and Public Health Ontario to monitor the epidemiology of HIV in Ontario and use that information to guide prevention, testing and engagement programs.
- The OHTN Cohort Study (OCS)—a database of clinical and social determinants of health data on an active cohort of about 4,000 people living with HIV in Ontario, which provides information to improve the quality, impact and consistency of HIV programs and services.
- OCHART (the Ontario Community-based HIV and AIDS Reporting Tool)—data on the prevention (education, outreach, community development), support and harm reduction services delivered by >100 community-based agencies across Ontario, which is used to meet accountability requirements and inform and strengthen programs.
- OCASE (Ontario Community-Based AIDS Service and Evaluation)—a case management tool used by 34 dedicated ASOs, which provide >85% of the community-based HIV support services across the province, to help understand health needs and the impact of services on health and quality of life.
Shifting our focus
Since its inception, the OHTN has been involved in collecting and analyzing data. We inherited the original HIV Ontario Observational Database (HOOD), which is now the OCS. At the request of the Ministry of Health and Long-Term Care, we developed OCHART in 2005 to help communitybased agencies report on their activities and OCASE in 2008 to give the province’s dedicated ASOs a case management tool. Just three years ago (2014), the ministry transferred the responsibility for monitoring the epidemiology of HIV (now the OHESI program) from the University of Toronto to the OHTN.
Data systems are challenging to maintain and operate. Database technologies have changed dramatically over the past 10 to 15 years, and a small organization like the OHTN can struggle to keep pace. At the same time, these technological developments offer the opportunity to gather data more efficiently, access data in real time and enable rapid learning at the point of care to guide clinical and organizational decisions.
Over the past two years, the OHTN has shifted both OCHART and OCASE to new platforms to make the systems easier, more intuitive and less time consuming for agencies to use and more helpful in terms of the timely information they can provide. Right now, we are looking at ways to modernize the OCS to ensure faster access to more timely, useful information. OCS data has contributed to a number of academic articles and has helped us understand the prevalence and impact of conditions that complicate HIV disease, such as hepatitis C, sexually transmitted diseases (STIs) and smoking among Ontarians living with HIV. However, to date it has had relatively little impact on HIV care in Ontario.
OHESI is a collaboration among the AIDS Bureau, the OHTN, Public Health Ontario (PHO) and the Public Health Agency of Canada (PHAC). PHO is responsible for collecting the data and maintaining the provincial laboratory databases. The OHTN’s Applied Epidemiology Unit focuses on analyzing that data and developing knowledge products that can be used to guide prevention and testing programs. HIV surveillance in Ontario has also been enhanced by investments made by the PHAC.
For example, for several years PHAC has funded the Laboratory Enhancement Program, which follows up with every physician reporting a new HIV diagnose to obtain information missing from the test requisition form (e.g., age, gender, ethnicity, risk factor). It is possible that this program could be enhanced to provide a better understanding of the factors driving new infections and the social networks most at risk.
To date, most of the OHTN’s investments in data analytics have been in systems and data collection. There has been relatively little capacity for data analysis and little effort to bring together data from across the different OHTN programs and from other sources to paint a more complete picture of Ontario’s HIV epidemic, the needs of the populations most affected, opportunities to improve the prevention, engagement and care cascade and Ontario’s progress (provincially, by region, by population and by clinic) in meeting the 90-90-90 targets. Over the life of this strategy, we will shift our focus from building systems and collecting data to making more effective use of existing data sources and conducting more comprehensive analyses. We will shift from identifying and measuring problems to: linking what we have learned about the health and social drivers of HIV in Ontario with evidence about how to influence those drivers; developing rapid learning processes that can drive change; and using data to monitor the implementation of those processes and measure their impact. The main goal will be enhancing prevention, engagement and care services.
The first steps
Over the next two to three years the OHTN will review all its data analytics programs to ensure they:
Enhance our understanding of emerging issues, including social determinants of health, comorbidities and aging, and the drivers of new infections.
The OHTN will strengthen its data analytics programs by:
- Restructuring the OCS to provide timely information to support the current and emerging challenges in clinical care.
- Exploring ways to use Institute for Clinical Evaluative Sciences (ICES) and other sources of data, such as patient reported outcomes, as part of rapid learning strategies to enhance care.
- Refocusing OCASE and OCHART on timely, relevant, in-depth data analyses that will support rapid learning and can drive change in ASO programs.
- Enhancing the range and depth of OHESI analyses and the accessibility and impact of OHESI cascade reports, profiles and related KTE initiatives to ensure that epidemiological information is used to enhance prevention and support programs.
- Exploring the potential to augment the Laboratory Enhancement Program.
- Developing comprehensive population-specific and regional profiles that, combined with effective rapid learning initiatives, will be used to strengthen prevention and support programs in all parts of the province.
2. Implement and assess care and service innovations.
The programs
The OHTN currently invests in three categories of research funding: project funding, funding for people (salaries) and board-directed funding.
Project funding is provided through four programs:
- The Impact-Focused Program funds projects that address priorities identified by the populations most affected by HIV and/or the prevention, engagement and care cascade.
- The Boys’ and Men’s Health team grants supports three Ontario teams focused on men’s health (funded collaboratively with the CIHR Institute of Gender and Health and CANFAR).
- The Community-Based Program provides small ($25,000) grants to front-line agencies to support program evaluation.
- The Indigenous initiatives support young Indigenous researchers to conduct projects that improve services and care in their communities.
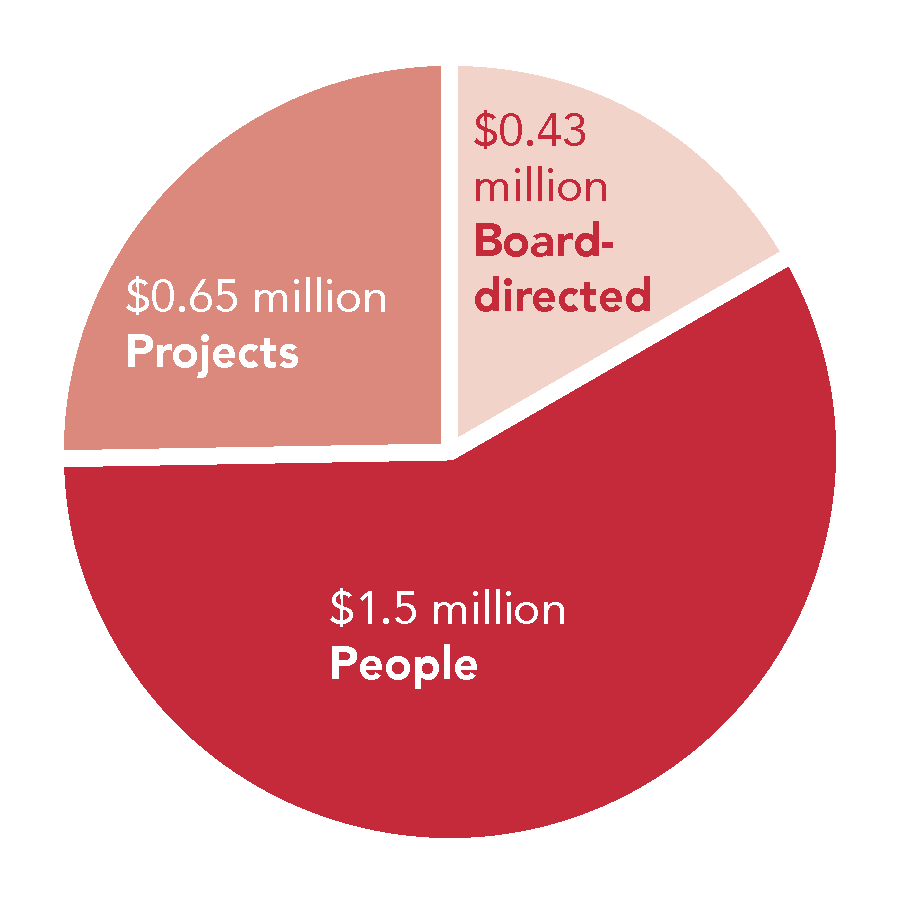
Funding by type
Funding for people is provided through four programs:
- The Impact-Focused Chairs Program provides five years of salary support to midcareer and senior scientists who champion innovative programs focused on a priority population or a key aspect of HIV care.
- Policy and Practice Leader awards provide salary support for clinical and policy leaders who will champion evidence-based practice among their peers.
- the New Investigator program funds two new investigators each year whose work will have impact on HIV prevention, engagement or care (peer review done by CIHR but fully funded through the OHTN).
- the OHTN Intramural Program provides salary and administrative support to a small group of in-house analysts who pursue external grants to explore topics relevant to the populations most affected by HIV and the prevention, engagement and care cascade.
Board-directed funds are used to support time-sensitive innovation on emerging issues, such as PrEP.
The OHTN supports project infrastructure including the community-based Research Ethics Board at the University of Toronto and the OHTN’s own Review Committees.
Shifting our focus
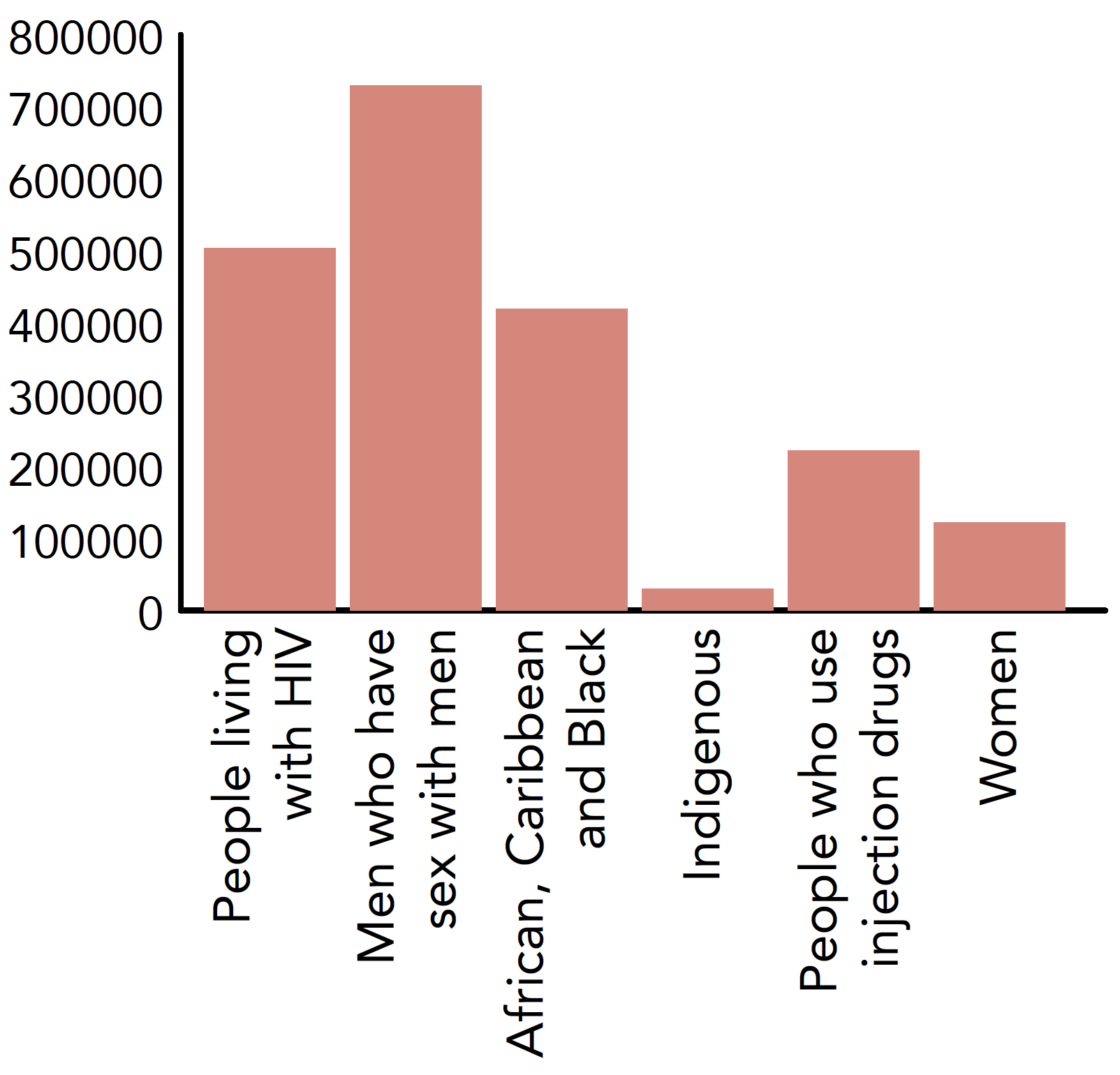
Over the past ten years, the OHTN’s funding programs have evolved from a traditional investigator-driven research program to a number of smaller funding programs designed to support the implementation of program innovations relevant to our stakeholders. We introduced our community-based program as a way to engage front-line agencies in assessing programs and move evidence into practice. About six years ago, we launched the Impact-Focused Program. To be eligible for funding, proposals had to address priorities identified by the OHTN in consultation with population-specific working groups. As this graph shows, a significant proportion of our funding is now focused on the health of gay men and African, Caribbean and Black communities.
Because of the lack of applications relevant to Indigenous health or with people who inject drugs, the OHTN has had to look for other ways to support that work, such as grants for emerging Indigenous researchers to undertake projects with an organization and direct support for feasibility studies of integrated supervised injection services in Ontario.
Over the past few years, the OHTN has invested more in people than projects. Some projects have been more effective than others in identifying solutions to problems and in creating pragmatic broadly-applicable programs and services. In 2015, the OHTN introduced the Ontario Engagement Accord, which sets out expectations about how the people we fund will collaborate with community and front-line service providers and with other OHTN programs to move evidence into practice.
Funding by Priority Population 2017-18
Over the past few years, most of our funding has been invested in multi-year chair and team grants. As a result, the OHTN has had little capacity to respond to emerging priorities or support innovative time-limited projects that could deliver new, more effective services. There has been no open call for projects since 2014. There have also been no programs to help engage young leaders in service and care improvement.
Over the next few years, the OHTN will continue its shift to more solution-focused implementation of interventions that can improve health care services and social supports for people living with and at risk of HIV.
Measuring impact
Cumulative complementary investments may have more impact than one-time grants. For example, it is possible to argue that a number of small OHTN investments, such as funding to investigate and evaluate the role of anal cancer screening for people with HIV, training for people to do anoscopies and equipment grants made it possible for a team, led by Dr. Irv Salit, to obtain a large federal grant. Ultimately this work has led to clinical guidelines and recommendations related to anal cancer screening, and impacts on practice and outcomes in Ontario. The teams’ work also contributed to a summary of the evidence that supported the introduction of the HPV vaccine for gay men and people with HIV.
Recognizing that service providers and policy makers work to tight timelines, we will endeavour to shorten the three to five years required (from idea through grant application to fundings and results) for traditional evaluation projects. Instead, we will try to spark rapid implementation approaches that answers key questions for the health system in a rigorous way.
We will encourage project teams to work closely with ASOs, testing programs, clinicians and policy makers to gain insights and evidence about what is needed to improve health outcomes; and to develop processes that can drive change. We will evaluate the impact of existing innovative programs and initiatives and work to disseminate these models. The OHTN will also develop consistent ways to ensure that any project that it funds meets the criteria for investment listed above.
First steps
Over the next two to three years the OHTN will critically review all existing funding programs against its criteria for investment (particularly criteria 1 and 4).
The OHTN will identify rapid learning implementation priorities for the 4th decade of HIV, focusing specifically on:
- Identifying the type of interventions required at this stage in the epidemic, to drive both local change and contribute to global knowledge (e.g. interventions to address the social drivers of HIV).
- Assessing the potential to conduct rapid evaluations of care and services (i.e. identify rigorous ways to answer critical questions in a short period of time).
- Establishing a process to set and continually review priorities.
- Determining how best to support emerging HIV leaders and analysts, particularly those from racialized communities.
- Forging new partnerships with other funders, universities and hospitals to make the best use of evaluation resources.
- Developing an effective way to measure adherence to the Ontario Engagement Accord, which sets out expectations about how innovators and the OHTN will collaborate to move evidence into practice.
Work with the Ontario Aboriginal HIV/AIDS Strategy (OAHAS) to identify best practices in data collection and evaluation to support Indigenous programs and services across Ontario.
Support the use of the best available data and evidence
One of our key roles in Ontario’s HIV sector is to drive change: to connect our partners with data and existing research evidence in a form that they can use for rapid learning that shapes more effective programs and services. In addition to providing evidence in accessible forms, we offer capacity building initiatives that help individuals and organizations develop the skills to integrate evidence into policy or practice. Now that we are at the endgame, our collaboration and rapid learning activities become the most critical pieces on the board. They are the difference between evidence that stays on the pages of a respected journal and the knowledge (i.e. a combination of evidence, frontline experience and capacity) and activities that change practice in ASOs, clinics and other parts of the health system.
The programs
The OHTN currently has multiple initiatives designed to help move knowledge into practice, including:
- A systematic review team and rapid response program that review, assess and summarize the literature.
- A requirement that knowledge users be part of all funded evaluation projects and teams.
- Knowledge repositories and products that make existing research findings and summaries available in formats that our stakeholders can use.
- Support for ASOs and other stakeholders who want to adopt/adapt evidence-based interventions.
- Knowledge-sharing events such as conferences, policy roundtables and think tanks.
The OHTN also supports a number of education and capacity-building programs, including:
- The Evidence-based Practice Unit which works with ASOs to enhance their capacity to evaluate their programs and services and adopt evidence-based practices.
- Clinical education initiatives, including quarterly meetings of the HIV clinic network and an annual pharmacy day, which strive to enhance clinical capacity.
- The HIV Residency Program and our specialized training for clinical care providers.
Shifting our focus
The OHTN has a strong commitment to engaging community and frontline care givers in building capacity in our sector. These stakeholders are involved in all OHTN-funded projects, and teams must have a detailed plan for how they will engage stakeholders and move findings into practice It is now time to integrate these assets to inform rapid learning across the HIV sector and to drive continuous quality improvement.
Our rapid response program is highly valued by those who have used it. Our conferences also score extremely high on evaluations – largely because they address specific Ontario issues, focus on the implications of research for policy and practice, include practice knowledge as well as research knowledge, and are accessible to all our stakeholders. There is growing demand from ASOs for assistance with program evaluation. By providing this support centrally, the OHTN makes these skills widely available across the sector and reinforces the importance of continuous quality improvement through ongoing monitoring and evaluation.
Quality improvement in our sector is an ongoing learning process that the OHTN is already a part of. For example, the OHTN and the Ontario AIDS Network (OAN) collaborated to develop an education program for ASO support workers linked to the October 2016 conference, HIV Endgame: Closing the Gaps in HIV Care. As part of that program, support workers met with coordinators from the HIV clinics to talk about how to work together to change the course of the prevention, engagement and care cascade. The OHTN also recently worked with the AIDS Bureau to organize a joint meeting of clinics and ASOs to discuss their roles in the new strategy and opportunities to develop local networks of integrated services.
The OHTN supports the Ontario HIV Clinic Network: a community of practice that comes together four times a year to discuss emerging clinical issues and identify education needs. That group now routinely monitors and reports on indicators such as number of patients retained in care, number lost to follow-up, number on treatment and virally suppressed, and strategies to keep people engaged in care. The OHTN is currently working with clinicians to launch guidelines for organizing and delivering HIV care that will encourage greater consistency across the province and help make the case for interdisciplinary care teams.
In terms of supporting the implementation of evidence-based interventions, the OHTN’s experience working with front-line providers (i.e. couples HIV test counselling, motivational interviewing and a prevention intervention for ACB women living with HIV) has reinforced the need for funding support for implementation science which, to date, has not been a priority within the OHTN budget. These experiences also illustrate the importance of context, feasibility and sustainability as service settings may not have the right skills or the resources to implement certain interventions. Over the next few years, the OHTN will shift its KTE focus, putting less emphasis on responding to requests for evidence and more on developing processes that will put knowledge into the hands of the right people and give them the tools to integrate it into practice. We will build on the idea of a rapid learning health and social system offering support for decision-making at partner organizations with timely and useable evidence, and fostering a culture of continuous learning and improvement in our sector. Instead of trying to share all HIV data and evidence, the OHTN will identify the data analyses and research findings that are most useful in the Ontario context (both its epidemic and its health system) and most likely to have an impact.
We will acknowledge that we are not the only organization with a role in education and capacity building for ASOs and work to define our role and priorities within that larger network (as we did with our recent collaboration with the OAN). The OHTN will play an active role in HIV Resources Ontario and work with other organizations to drive change. Our role will focus on providing data and evidence and on supporting evidence-based decision-making within our sector.
Over the next five to 10 years, the most pressing challenge in clinical care will be the large number of HIV clinicians retiring. The OHTN, in collaboration with clinics and health sciences schools, will pursue new approaches to attract clinicians to the field and provide the evidence, education and support they need to be confident providing HIV care.
The first steps
Over the next two to three years the OHTN will evaluate the impact of all KTE and capacity-building initiatives, based on our criteria for investment and involvement (particularly criteria 1, 2 and 3).
To strengthen our capacity to support rapid learning and continuous quality improvement in the HIV sector, the OHTN will:
- Define our role in learning and capacity building as part of a network of provincial capacity-building organizations.
- Establish rapid learning and capacity building priorities based on our stakeholders’ needs and taking into account the results of our evaluations and the skills and expertise required.
- Develop rapid learning approaches that are tailored to specific audiences (e.g. ASOs, clinicians, policy makers).
- Explore the potential to be an incubator for practice innovations. To help Ontario meet the 90-90-90 targets, the OHTN could actively support clinic and ASO efforts to quickly implement and evaluate new programs or practices, and scale up those that are effective.
- Develop a plan and a budget to support program science-driven interventions. If Ontario is to benefit from what we already know about evidence based interventions, it will be important to re-allocate funds from other OHTN programs to create a budget for this program.
- Identify more effective ways to leverage the findings from rapid syntheses so they can be used to strengthen programs and services.
- explore alternatives to large conferences to share information, build communities of practice, change programs and services, and improve health outcomes.
Help create the backbone for collective impact in the HIV sector
The Program
The OHTN is one of a group of provincial backbone resource organizations that support the vibrant network of front-line HIV services in Ontario (see Appendix A.)
Shifting our focus
In 2003-04, the AIDS Bureau sponsored a community planning exercise that brought together services within a region to create an HIV plan. As part of that exercise, provincial organizations also met but were unwilling to move beyond traditional partnerships in their work. More than 10 years later, there may be an opportunity to forge a more integrated working relationship.
Collective impact is a social change theory that involves bringing together a broad network of agencies and organizations to solve complex social problems such as HIV. To be effective, organizations using the collective impact approach must:
- have a common agenda
- collect data and measure results consistently
- undertake mutually reinforcing activities
- maintain open communication
- have a backbone organization that can coordinate and support participating individuals and organizations.
Ontario’s HIV sector already has many of the pieces in place to achieve collective impact. Ontario now has a common agenda and more direction about mutually reinforcing activities. The sector has a long history of open communication and, in recent years, a much stronger commitment to collect data and measure the impact of its work. In 2016, the provincial resource organizations came together to create HIV Resources Ontario, a forum where they can work together to coordinate their support for ASOs. They have already developed a single web site where community-based organizations can go to find all the resources available to them and how to access them. They are developing ways to jointly deliver trainings and workshops that meet ASO needs.
To reach and win the endgame, the OHTN will champion the collective impact approach. Over the next 10 years, the OHTN will shift from operating somewhat in isolation to working much more closely with the AIDS Bureau and other provincial resource organizations to form the backbone for Ontario’s HIV sector. The OHTN will take the lead in analyzing data and measuring results, and will negotiate with the other backbone partners how it can best contribute to the other activities (i.e. mutually reinforcing activities, open communication, coordinating and supporting participating organizations).
To determine its role in the backbone, the OHTN will use its criteria for investment and involvement, focusing particularly on criteria 2 and 3.
The first steps
Over the next two to three years:
- The OHTN will establish its role as part of the HIV backbone by:
- Providing data and evidence to drive change as well as monitoring and evaluation to measure impact.
- Forging a stronger relationship with the other provincial backbone organizations to define roles in driving change (e.g. memorandum of understanding).
- Establishing ways to work together that avoid unnecessary duplication.
- Identifying opportunities to share resources and expertise to undertake mutually reinforcing activities, develop more effective tools and resources, and achieve common goals.
- As part of collective impact, the OHTN will:
- Explore the potential to develop integrated products, establish shared administrative services (e.g. finance, HR) and co-locate some services.
- Forge stronger relationships with other sectors beyond HIV including public health (to increase the reach, timeliness and accessibility of targeted testing programs) and mental health and addictions (to improve access to care all along the prevention, engagement and cascade).
4
“A backbone organization requires dedicated staff who can plan, manage, and support the initiative through ongoing facilitation, technology and communications support, data collection and reporting, and handling logistical and administrative details. … In the best of circumstances, backbone organizations embody the principles of adaptive leadership: the ability to focus people’s attention and create a sense of urgency, the skill to apply pressure to stakeholders without overwhelming them, the competence to frame issues in a way that presents opportunities as well as difficulties, and the strength to mediate conflict among stakeholders.”(Kania and Kramer, 2011)
Structuring the OHTN for the 4th decade of HIV
The OHTN’s new strategic directions demand different organizational structures, resources and approaches. To be able to make the tactical moves required to reach and win the endgame, the OHTN must assess whether it has the appropriate structure, people and skills and address any gaps. We must also support staff to work in a rapidly changing and responsive environment, create a healthy workplace and provide timely opportunities for professional growth and career advancement. We must also engage staff and listen to their feedback on how we can reach and win the HIV endgame.
The OHTN will develop an operations plan and an HR plan to support the strategic plan.
The OHTN board will engage in portfolio management to ensure that the organization provides exceptional value for money. Three key governance groups will be essential to the process of portfolio management:
- Innovation Advisory Committee will play a key role in ensuring our criteria for investment are applied to all our data, research and learning programs.
- Finance Committee will play a key role assessing value for money.
- Executive Committee will play a key role in overall management of the OHTN’s portfolio.
Accountability: focusing our efforts, monitoring our progress and evaluating our impact
The OHTN’s Strategic Plan sets out directions for the next 10 years. The actual activities—our priorities each year—will evolve over time and be laid out in three-year operational plans and in annual program plans. We will also revisit our strategic directions every three years to ensure that they are having a measurable impact and achieving the desired outcomes.
Using the 90-90-90 targets and the other metrics that will be developed, we will continuously monitor and track our progress. We will be able to see whether we are realizing our own vision and mission as well as helping to achieve province-wide goals.
Each year, we will report to our Board and to the AIDS Bureau on our part in province-wide efforts to meet or exceed the 90-90-90 targets and to achieve the goals of the HIV/AIDS strategy for Ontario.
Because we are responsible for many data systems for the sector including epidemiological data, clinical data and community-based data—we will also help all parts of the sector measure and monitor their work.
5
“The AIDS movement, led by people living with and affected by HIV, continues to inspire the world and offer a model for a people-centred, rights-based approach to global health and social transformation. And yet, today… we confront a serious new obstacle: the oppressive weight of complacency. This is happening when we know that if we make the right decisions and the right investments now, the end of AIDS can be within our grasp. This moment is, however, fleeting. We have a fragile window of opportunity—measured in months—in which to scale up.”On the Fast-Track to end AIDS, Michel Sidibé, Executive Director, UNAIDS
The next—last?—decade
We stop AIDS—we reach and win the endgame—only when we are willing to work together and work differently. If we accept business as usual, we will continue to have:
- about two new HIV diagnoses each day
- people with HIV dying too young
- too many people with or at risk of HIV living in poverty, experiencing discrimination or
- struggling with undertreated mental health and addiction issues.
We will also lose the current opportunity created by global targets, provincial policies, and advances in HIV treatment and prevention.
The OHTN is committed to upping our game. We see a time when HIV is no longer a threat and the OHTN—as well as many other HIV programs and services—are no longer needed.
Over the next 10 years, we will collaborate closely with other provincial resource organizations to form the backbone for the sector. We will work differently, continually looking for effective ways to use our resources to achieve common goals. We will support rapid learning in our sector, collaborate closely with our partners to support the use of high-impact data analyses and research evidence—providing information in a form they can use—and help them develop their capacity for evidence-based decision-making.
Our game plan will help Ontario’s HIV sector develop the skills, knowledge and resources to provide the kind of evidence-based policies, programs and services that will make the fourth decade of HIV/AIDS the last.
Appendix
Backbone organizations supporting effective action in the HIV sector
- The AIDS Bureau provides strong policy direction and funding.
- The OHTN provides and supports the use of data and research evidence, as well as providing capacity building for people with or at risk of HIV, ASOs, HIV clinics, policy makers, researchers and others involved in the work.
- The Ontario AIDS Network (OAN), the association of community-based AIDS service organizations (ASOs) in Ontario, provides training for ASO staff and a voice for the community-based sector.
- The Ontario HIV Clinic Network (OCN) provides a forum for the provinces’ HIV clinics to share information and keep up to date on HIV care.
- CATIE (Canadian AIDS Treatment Information Exchange) provides information on HIV and hepatitis C for the community.
- The Ontario Organizational Development Program (OODP) provides expertise and resources to support community-based ASOs.
- The priority population networks help community-based organizations focus on the populations most at risk:
- The Gay Men’s Sexual Health Alliance (GMSHA) develops awareness campaigns and other resources to support HIV prevention efforts.
- The African and Caribbean Council on HIV in Ontario (ACCHO) develops awareness campaigns and other resources to help meet the needs of African, Caribbean and Black communities.
- The Women and HIV/AIDS Initiative (WHAI) works with other agencies that serve women to make them more aware of the needs of women with HIV.
- The Committee for Accessible AIDS Treatment (CAAT) works with HIV and other services to meet the needs of immigrants, refugees and people without status.
- The Ontario Aboriginal HIV/AIDS Strategy (Oahas) develops the HIV/AIDS strategy for Indigenous peoples in Ontario and has education and prevention workers in agencies across the province.
- The Ontario HIV and Substance Use Training Program (OHSUTP) provides training for addiction agencies that work with people with HIV to make them more aware of their needs.