Questions
What structural, process, and outcome measures are used to monitor and evaluate the impact of supervised consumption services (SCS)?
Key take-home messages
- A 2019 systematic review identified several types of outcomes from scientific literature that guide assessment of SCS, including: usage by high-risk individuals, safe injection practice, overdose management, uptake of treatment and other healthcare services, decreased public drug use, prevention of blood-borne diseases, and decreased crime (1).
- There are several services that occur at SCS, including, but not limited to: access to sterile drug use equipment (2), drug-checking services (3, 4), hepatitis C testing, treatment, and care (5, 6), hepatitis B vaccination (7), risk-reduction education (8), and testing for HIV and other sexually transmitted infections (2). These SCS processes can be evaluated by the outcome measures proposed in the aforementioned systematic review (1).
- Various study designs employing different types of data were used to evaluate SCS outcomes: ecological studies, modelling studies, prospective cohorts, and cross-sectional surveys (1).
The issue and why it’s important
Canada is currently in the midst of an ongoing opioid epidemic (9), where 17,602 apparent opioid toxicity deaths occurred between January 2016 and June 2020 (10). Between April and June 2020, 1,628 apparent opioid toxicity deaths occurred, representing the highest quarterly count since national surveillance began in 2016 (10). This number also represents a 58% increase compared to January to March 2020 (1,029 deaths) and a 54% increase from the same time frame in 2019 (1,059 deaths) (10). In 2020 (January to June), 97% of apparent opioid toxicity deaths were accidental (i.e. unintentional) (10).
One way the Canadian government is addressing the opioid epidemic is by approving supervised consumption sites and services (9, 11, 12), also known as supervised injection facilities (12), medically supervised injection centres (12), and drug consumption rooms (1). Policy reform at the federal level in Canada in 2017 led to an increase in the number of sites: Bill C-37 was passed, which reduced the number of criteria that sites needed to meet in order to be granted an exemption (11).
To legally operate in Canada, a site offering SCS must apply for an exemption under section 56.1 of the Controlled Drugs and Substances Act, which describes exemption for medical purposes at a supervised consumption site (13). The first legally sanctioned supervised drug injection site in North America, Insite, opened in 2003 in Vancouver (14). As of January 2021, there are 37 SCS operating in Canada that hold valid exemptions (15). According to the National Harm Reduction Coalition, there are more than 100 SCS located in over 60 cities in 11 countries worldwide (16), including Germany, the Netherlands, Switzerland, Spain, Canada, and Australia (1).
SCS are set up in areas of higher public drug use (17). These sites are safe spaces supervised by trained staff where individuals can, depending on the site (15), inject, inhale, swallow, and/or snort pre-obtained drugs with sterile equipment (2). SCS may also provide access to health and social services, such as: testing for infectious diseases, education on the harms of drug use and safe consumption practices, access to medications to treat opioid use disorder, and mental health treatment (17). Research has also shown that SCS enhance access to primary health care for people who use drugs (18), a meaningful aspect of SCS, as research demonstrates that people who inject drugs may face barriers when accessing medical services (19-21). Additional ancillary services may be provided at SCS, including employment programs, laundry facilities, peer support programs, and recreational activities (22). Other services typically offered at SCS in Canada include monitoring for signs of overdose, and naloxone distribution and training (2). Some sites also offer authorized drug checking, a harm reduction measure where drugs are tested for toxic or potent substances, such as fentanyl (15).
In addition to SCS, in Canada there are overdose prevention sites where peers or other (typically non-nursing) staff can monitor people who have used drugs for signs of overdose (2). When an overdose occurs, there can be rapid intervention using naloxone or providing oxygen if needed (2). In December 2017, Health Canada gave all provinces and territories the ability to apply for a class exemption and be granted the power to approve temporary (three to six months) overdose prevention sites based on urgent need, without requiring the same application process to receive an exemption from federal drug laws for an SCS (2). This review explores some of the structural, process, and outcome measures used in the literature to evaluate the impact of SCS (1, 23–25).
What we found
Understanding healthcare measures
Generally, data are collected information, such as facts or numbers, that are examined and used to guide decision-making (26, 27). Data can be broadly classified as either quantitative or qualitative (28, 29). Quantitative data can be collected from surveys, questionnaires, or equipment, among other methods; these data are measurable, precise, and objective, and can be utilized numerically (30). Qualitative data can be collected from interviews or observations, among other methods; these data enhance the understanding of the phenomenon, and are comprised of words, behaviours, or images (30). A range of data — including qualitative and quantitative — are needed to understand the quality of care provided or received, and how a healthcare service is performing (27). Additionally, several sources of data — such as medical records, patient surveys, and administrative databases (31) — are needed to understand how a complex system in healthcare performs (27).
The collection and analysis of healthcare data allow for effective reporting of health outcomes (32, 33). In simple terms, health outcomes are changes in health that result from a specific healthcare intervention or investment (32). Veillard et al. (2015) note that “…outcome measures help better understand how…healthcare services can contribute to achieving targeted outcomes and their role in the broader social determinants of health” (34).
Our understanding of using outcomes in healthcare can be attributed to Avedis Donabedian (27, 35), a founder of the study of medical care organization and health service quality (36). Donabedian discussed the necessity of focusing on structures and processes in order to improve health outcomes (23–25, 27):
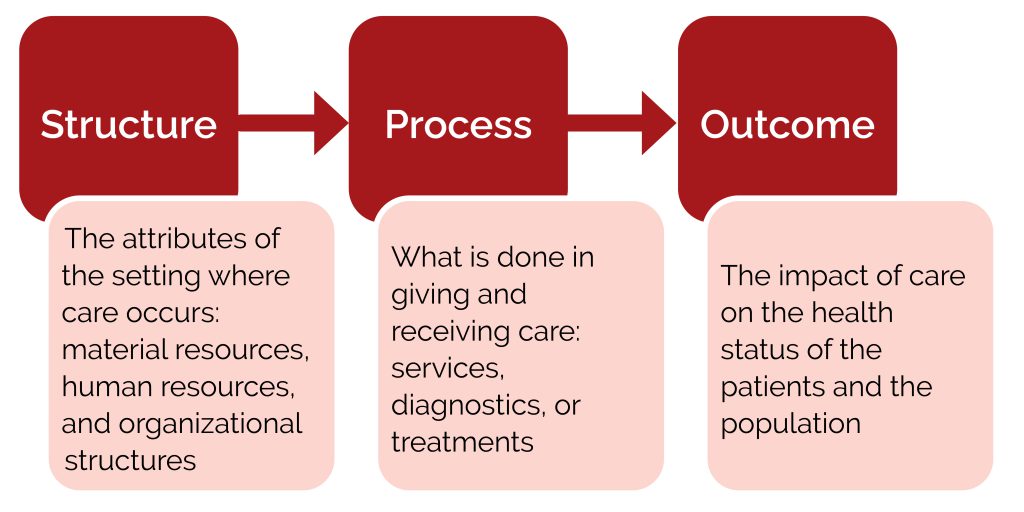
Figure 1: The Donabedian model for quality of care (23–25)
In this model, Donabedian suggests that structure impacts process, which in turn affects the outcome (23–25).
This model of structure, process, and outcome is considered to be the best-known framework in health services research (35), and is foundational to quality assessment (36). An influential report published in 1990 by the Institute of Medicine, which drew extensively on Donabedian’s work (36), defines quality of care as “…the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge” (37). More simply put, quality of care is achieving better health outcomes for people (38). The next section of this review examines structure, process, and outcome measures in the context of SCS.
Structure and process measures at SCS
Structure refers to the characteristics of the setting where care occurs: this includes the facility, its location, organizational structure, operating times, and the staff and their qualifications (23, 25). An operational guidance report for SCS produced by the BC Centre on Substance Use (BCCSU) states that:
“[t]here are different ways to plan, design, and implement a SCS and, accordingly, many issues to consider with respect to the target client population, existing network of services for PWID [people who inject drugs], and resources available, including funding, space, and staff. Need should be determined through relevant environmental scans, needs assessments, and feasibility studies” (22).
The following studies are some examples of research conducted in line with the above suggestions.
One study from 2017 examined acceptability, design, and operational preferences for a supervised injection service in London, Ontario (39). Peer research associates administered a survey among people who inject drugs, that collected data on willingness to use the site and site preferences, including: site location, willingness to walk or take public transit to the service, hours of operation, involvement of peers, and layout of the injecting space (39). Results from the survey demonstrated that the most important amenities were “…distribution of sterile injecting equipment, preventing and responding to overdoses, needle distribution, HIV/HCV testing, and washrooms” (39). Of those who reported a willingness to use a supervised injection service (n=170; 86%), 82% were willing to use a service integrated into a community health centre, hospital, doctor’s clinic, or social service agency; 84% preferred private cubicles as a set-up; 73% preferred daytime hours of operation; and 49% reported that peers should be involved in operation of the service (39).
Another study consulted with people who use drugs and other community stakeholders from Ottawa and Toronto to examine how supervised consumption facilities should be designed (40). Other community stakeholders included first responders, healthcare providers, city officials, city employees, residents, and business owners (40). Between December 2008 and January 2010, 26 key informant interviews and 28 focus group discussions occurred: 95 individuals who use drugs (32 in Ottawa, 63 in Toronto) and 141 other community stakeholders (80 in Ottawa and 61 in Toronto) were consulted (40). Compared to the other community stakeholders, people who use drugs offered detailed responses on how a facility should be designed (40). When questioned regarding facility design for supervised injection and supervised smoking, people who use drugs had a strong preference for separating supervised injection and smoking into different rooms within a facility (40). Desire for physical separation between the two different types of consumption was based on: two different highs, comfort regarding exposure to different methods of drug administration, and concerns about behaviours associated with smoking crack cocaine (40). Other community stakeholders were less vocal about design issues compared to people who use drugs, but raised three potential implementation challenges for supervised smoking facilities: political resistance, tobacco smoking bylaws, and preventing staff exposure to second-hand smoke (40). Of note, a scoping review published in 2020 described existing SCS models from other high-income settings that accommodate other routes of consumption for drugs that are taken orally, intranasally, or via inhalation (41). A quasi-experimental study in Barcelona, Spain examined the impact of a 24-hour schedule of a drug consumption room on service use and number of non-fatal overdoses (42). Authors compared the client profile, facility use, drugs used, and the number of non-fatal overdose episodes in different timeframes: a 15-hour opening period (March–June 2018) and a 24-hour opening period (July–October 2018) were compared with each other, and daytime and nighttime were compared during the 24-hour period (42). Sociodemographic data were collected during both 15-hour and 24-hour opening periods, and for daytime and nighttime client groups (42). While authors found that there were no sociodemographic differences between the clients in the 15-hour and 24-hour periods, authors did find a difference between clients who used the service during the day and those who used the service at night (42). During nighttime, there was a higher proportion of women and homeless people who used the service, compared to the daytime (42). Additionally, cocaine use was more frequent at night, and injected heroin use was decreased (42). A non-statistically significant increase in non-fatal overdose was observed during nighttime; however, when heroin use was examined alone, this increase became statistically significant (42).
Process can be described as what is actually done in giving and receiving care: this includes the activities of the individual in seeking care, and the healthcare provider’s role in diagnosing and implementing treatment (25). At SCS, this includes access to sterile drug use equipment, a place to safely dispose of needles, and emergency medical care to address overdose, allergic reaction, or cardiac arrest (43). The aforementioned operational report produced by BCCSU notes that “…[t]he type, range, and scope of services offered depend on the client population’s characteristics and needs, existing local services, and resources available to establish a facility” (22).
Additionally, a scoping review examining rules and eligibility criteria for SCS feasibility studies concluded that best practices for SCS service delivery must be established in order to address implementation issues and increase access for clients (44). The operational report produced by the BCCSU provides a list of 22 ancillary services — or processes — that an SCS may provide, noting that this is dependent on the “…needs of the client population, existing services available in the area, and overall budget and capacity of the facility” (22). These ancillary services, among others, include: health education, including harm reduction strategies for drug use, drug-use related medical care (e.g. wound care, vein care, abscess management); primary care (e.g. immunization, STI screening, screening for other communicable diseases such as HIV and hepatitis C); naloxone provision and training; residential services (e.g. overnight shelters, residential nursing care); employment and peer support programs; meals; shower; laundry; and overnight shelter (22). Some examples of the varied processes occurring at SCS at different settings around the world are described below. Outcome measures are reported in brief at the end of each paragraph.
Drug-checking
Drug-checking is a harm reduction intervention where individuals can test the composition of their street drugs, allowing for informed decision-making (4, 45). In British Columbia, fentanyl test strips are provided at all SCS and overdose prevention sites (3). At Insite in Vancouver, the goal of the drug-checking service is “…to improve clients’ awareness of their exposure to fentanyl and improve our understanding of the drug supply” (4). A 2018 study from Insite found that from July 2016 to June 2017, only a small proportion of visits resulted in a drug-check (1%); however, approximately 80% of the checked drugs were contaminated with fentanyl (4).
In Toronto in 2019, a network of drug-checking services was launched, co-located within SCS at three frontline agencies (46). A forthcoming study, published as a protocol in 2020, will evaluate the impact of drug-checking services on: changes in and factors influencing overdose and related risk behaviours, perceived capacity to prevent overdose, and drug composition trends in Toronto (46). In particular, the study will evaluate: the impact of access to drug-checking services on self-reported overdose; the proportion of participants reporting increase in protective behaviours (not using alone, carrying naloxone, use of SCS, consultation with staff, smaller dosage, discarding toxic substances); the proportion of participants reporting they gained, intend to use, and/or used knowledge and skills (46). The study will also investigate: facilitators and barriers to the use of drug-checking services, and the number of analysis results detecting composition different from participant expectations (46).
Hepatitis B vaccination
A study in Germany outlines the implementation and success of administering the hepatitis B vaccine to people who inject drugs attending a drug consumption facility in the city of Essen (7). This facility is part of a larger health care centre that offers drug counselling, an opioid maintenance clinic, and a night shelter for homeless individuals (7). Hepatitis B serology testing was offered to clients regularly attending the drug consumption facility who reported no history of hepatitis B infection or vaccination (7). The vaccination schedule was coordinated by a social worker, and staff members made efforts to ensure completion of the three-dose vaccination (at 0, 1, and 6 months) (7). Of the 64 clients who were suitable for vaccination, 58 (90.6%) received at least one vaccination, 56 (87.5%) had two vaccinations, and 47 (73.4%) completed all three vaccinations (7).
Hepatitis C testing
Clients of SCS typically have high hepatitis C infection rates, and most SCS provide hepatitis C testing on-site (5). Results from an international survey completed by managers of 91 SCS found that the availability of onsite medical professionals, in addition to supporting and educating non-medical staff, are vital to hepatitis C support and treatment (5). At Moss Park Consumption and Treatment Service (MPCTS), a nurse from the Toronto Community Hepatitis C Treatment Program comes weekly to run a three-hour clinic and performs hepatitis C testing, in addition to delivering treatment to existing patients (6). In the first six months of the program at MPCTS which began in 2019, 32 individuals engaged in hepatitis C testing; of these, 13 tested positive (6). Five of these 13 individuals initiated treatment (6).
Risk-reduction education
An intervention offered at eight SCS in France provided face-to-face educational sessions about HIV and hepatitis C risk reduction and safer injection practices (8). The sessions were delivered by doctors, nurses, psychologists, social workers, and peers, and included counselling about safer injection, direct observation of injecting practices, and shared discussion (8). Results demonstrated that participants of the intervention were more likely to improve in these drug-use steps: hand washing, skin cleaning, setting up a sterile preparation area, and post-injection bleeding management (8). Authors noted that this intervention was inexpensive, easy to implement, and was effective in reducing certain unsafe drug-injecting behaviours (8).
Take-home naloxone
The Sydney Medically Supervised Injecting Centre (MSIC) in Australia introduced a take-home naloxone program in January 2015 (47). Staff at the MSIC are trained to deliver individual-level, brief interventions lasting 10-15 minutes (47). While this program is alluded to in peer-reviewed literature (47, 48), there does not appear to be a robust report detailing the processes of this program. A presentation of this service notes that a brief, 5–10 minute, intervention was developed, followed by a Memorandum of Understanding with the local pharmacy, creation of naloxone packs, and a no-barrier approach to replacement (49). Ninety clients were trained and provided with naloxone packs, and 13 overdose reversals were recorded (49, 50).
Outcome measures at SCS
A systematic review published in 2019 by Belackova et al. sought to address evaluation methodologies of drug consumption rooms and supervised injection facilities (1). This review (1) describes eight broad types of outcomes identified in the literature (18, 51-55). Note that the five services described in the previous section on process (drug checking, hepatitis B vaccination, hepatitis C testing and treatment, risk-reduction education, and management of overdose) all have outcomes that can be classified using the eight outcome types identified by Belackova et al. (1):
i. attracting high-risk, marginalized users
ii. management of overdose and decreased mortality
iii. enhancement of safe injecting practices
iv. decreased public drug use and improved public amenity
v. increased uptake of treatment and other healthcare and social services
vi. prevention of transmission of blood-borne diseases and the associated economic benefits from it
vii. no increase in crime
viii. no increase in drug use or related risks.
Authors note that no existing literature review systematically described the methodology of SCS evaluation, or how it was used to assess specific outcomes (1). This systematic review explored evaluation methodologies for the above eight outcomes in grey and scientific literature published before June 2017 (1). Authors included 219 peer-reviewed articles published since 1999, including 56 studies reporting on evaluation outcomes; 117 articles were from Canada, 36 from Europe, and 32 from Australia (1). Authors note that included studies were highly skewed to one single facility in Canada, and one in Australia (1).
Various study designs were used to evaluate the outcomes: to assess the impact on overdose, public nuisance, and crime, ecological study designs (e.g. quasi-experimental, with pre-test and post-test assessments) were used; to examine the impact on blood-borne virus transmission, overdose deaths, and economic benefits, modelling studies (e.g. cost-effectiveness of supervised injection facilities in preventing blood-borne diseases, evaluating the number of averted fatal overdoses) were used (1). Finally, individual-level data collected from prospective cohorts, cross-sectional surveys, and service records were used to assess safe injecting practices, uptake of health and social services, in addition to the aforementioned outcomes (except for crime and costs) (1). Studies utilizing individual data employed different indicators of individual-level exposure in SCS (1).
Authors found that exposure to the intervention (i.e. the SCS) was measured by attendance, and this was done in four ways: as a dichotomized indicator for a specified time period (i.e. answering “yes”/“no”), a discrete indicator of the number of visits per client using service records (i.e. counting attendance), indicators of visit frequency (i.e. “attended more than twice per week”), and the proportion of injections that occurred at a facility from all injections (1). Belackova et al. classified outcome measures reported in 56 studies into eight different evaluation outcome types (listed above) (1). We identified additional studies published since the search date of Belackova et al. systematic review (June 2017) and, by adapting her classification model, provided a list of SCS outcome measures used in evaluation of the impact of SCS. These are summarized in Table 1.
i. attracting high-risk, marginalized users
A community-recruited cohort study in Vancouver collected data from people who inject drugs prior to initiating use at a supervised injection facility (Insite) to determine if the site attracted higher-risk individuals (i.e. those at greater risk of overdose and blood-borne diseases) (56). The collected quantitative data included gender, age, HIV status, involvement in sex trade, methadone use, injecting in public, difficulty accessing needles, borrowing used needles, unstable housing, daily heroin injection, daily cocaine injection, and recent non-fatal overdose (56). The authors found that the facility attracted those at elevated risk of blood-borne infections and overdose (56). Authors suggested that the supervised injection facility may have contributed to improved health outcomes among people who inject drugs by providing a hygienic environment and emergency response in case of an overdose (56).
ii. management of overdose and decreased mortality
A study published in 2011 found that overdose mortality in the immediate vicinity of Insite was reduced after it opened (57). Authors examined overdose mortality rates for the period before and after the opening, comparing overdose fatality rates within a 500-metre radius and the rest of the city (57). A 500-metre radius was selected because data from a previous study indicated that more than 70% of daily users lived within approximately four blocks of the facility (57). Of the 290 accidental, fatal drug overdoses that occurred between January 2001 and December 2005, nearly one-third (n=89) occurred in city blocks within 500 metres (57). In the examined period of September 2003–December 2005 (i.e. after the opening of the facility), the number of fatal overdoses in the 500-metre radius decreased by 35.0%, from 253.8 to 165.1 deaths per 100,000 person-years (57). During this same period, the fatal overdose rate in the rest of the city decreased by 9.3%, from 7.6 to 6.9 deaths per 100,000 person-years (57). Authors suggest that SCS should be considered where there is a high burden of overdose due to injection drug use (57).
A more recent study conducted in Toronto estimated associations between SCS use and recent non-fatal overdose among people who inject drugs (58). Authors collected baseline interview data between November 2018 and March 2020 from an ongoing, longitudinal cohort of people who inject drugs (58). Of the 701 eligible participants, more than half reported daily injection drug use (n=398; 56.8%) (58). Of the 695 participants who reported injection drug use in the past six months, the majority (n=601; 86.5%) reported injecting at an SCS, whether it be “all/most”, “some”, or “few” injections, and 13.5% of participants did not use SCS in the previous six months (58). About 39% (n=270) reported a recent overdose; of those that reported an overdose in the past six months, 20.5% (n=55) reported that the overdose took place at an SCS (58). Authors found that there was no statistically significant relationship between SCS use and non-fatal overdose, whether comparing more frequent SCS use to less frequent use or to no use (58). Although no comparisons were statistically significant, the point estimates and confidence intervals were consistent with potentially weak associations between regular SCS use (≥25% of injections) and non-fatal overdose (58). Authors suggest that this may support the hypothesis that unmeasured confounders, such as severity of substance use disorder, could have an impact on the relationship between SCS use and non-fatal overdose (58). Some studies restrict samples to only SCS participants in order to minimize the potential for bias in the sample (58, 59). For example, a study of 811 individuals from Vancouver found that frequent (at least weekly) use of a supervised injection facility was associated with a lower risk of death, independent of relevant confounders (59).
iii. enhancement of safe injecting practices
A 2008 study among individuals using a supervised injection facility found that the overall environment promoted the adoption of safer injecting practices over time, both within and outside of the facility (60). Authors identified three central themes that emerged from the interviews with 50 individuals recruited from a cohort of people who inject drugs in Vancouver (60). First, participants noted a general lack of knowledge regarding safer injection practices prior to attending the facility, something that was not limited to first-time injection drug users; furthermore, participants also discussed being unaware that they were injecting unsafely until they began using the site and received education regarding safer injecting practices (60). Second, participants noted that the site was the first place they had been able to successfully receive help – several visits to the facility for the primary purpose of consuming drugs resulted in receipt of educational messages that were accessible and reinforced over time (60). In addition, the nursing staff at the facility represented a source of information that was reliable and accurate compared to messaging received “on the street” (60). Finally, the provision of sterile syringes and other injecting equipment, paired with information from a trusted source, contributed to an atmosphere where participants were conscious of the safety messages, and diligent in putting them to practice (60).
iv. decreased public drug use and improved public amenity
A study from Australia examined community perceptions of the Sydney MSIC on community perceptions of public amenity (61). The authors’ objectives were to determine if public amenity changed over time, using data collected prior to the opening of the establishment of the MSIC (baseline), after 18 months (short-term), and after four years (medium-term) (61). Telephone surveys were administered randomly to local residents and business operators in the local vicinity of the MSIC at baseline, short-term, and medium-term (61). Respondents were asked about their perceptions and consequences of drug use in their neighbourhood, in addition to perceived advantages and disadvantages of the MSIC (61). At baseline, 515 residents and 269 businesses completed the survey; at short-term, 540 residents and 207 businesses completed the survey; at medium-term, 316 residents and 210 businesses completed the survey (61). When questioned about witnessing public injecting and publicly discarded injecting equipment, authors observed that among residents, there was a significant decrease in having witnessed public injecting and publicly discarded injecting equipment in the past month over the five-year study period (61). Additionally, over 90% of residents surveyed at medium-term reported at least one advantage to having an MSIC in the area; the top three were control of HIV/AIDS and hepatitis C, reduced overdose risk, and reduced number of drug users on local streets (61).
v. increased uptake of treatment and other healthcare and social services
Some research has indicated that SCS may promote increased uptake of addiction treatment and subsequent cessation of injection drug use (62). To further examine this, one study characterized the use of detoxification services co-located at Insite (63). Called Onsite, this detoxification service has operated since 2007 (63), and currently includes a 12-bed detox floor and an 18-bed transitional housing floor (64). Additionally, a range of recovery-oriented programs alongside health and housing supports are offered (64).
The primary outcome of the study was reporting enrollment in on-site detoxification services in the past six months (63). Using data from two prospective, ongoing cohorts of people who use illicit drugs in Vancouver (n=1,316), authors selected a variety of sociodemographic and behavioural variables to include in their analysis, including: age, gender, ancestry, sex work involvement, housing status, residence within five blocks of the facility, daily drug injection practices, non-fatal overdose, public injecting, syringe sharing, and frequent SCS use (63). To determine factors potentially associated with accessing on-site detoxification services, authors used a statistical approach known as general estimating equations (63). The study found that over 10% of the sample reported accessing on-site detoxification services over the two-year study period (63). Furthermore, living less than five blocks from the facility, participation in methadone maintenance therapy, public injection, binge injection, and frequent SCS use were independently associated with reporting use of detoxification services at Insite (63). When this sample was restricted to individuals who reported recent use of the SCS (n=554), 23.7% (n=131) reported accessing detoxification services over the two-year study period (63).
vi. prevention of transmission of blood-borne diseases and the associated economic benefits from it
A 2016 study estimated how cost-effective it would be to establish one or more supervised injection facilities in Toronto and Ottawa, taking into account HIV and hepatitis C infections, averted cost of prevented infections, geographic distribution of drug use, self-reported willingness to use a facility, and cost to operate a facility (65). Health effects were quantified by the number of potentially averted HIV and hepatitis C infections, and the number of quality-adjusted life-years gained (65). Over 20 years, it was projected that one facility in Toronto would avert 164 HIV infections and 459 hepatitis C infections, for a net savings of CAD 9.6 million when compared to no facility (65). In the case of Ottawa, one facility would avert 358 HIV infections and 323 hepatitis C infections, for a net savings of CAD 0.8 million (65). Authors noted that the main health and financial reductions accrued from the supervised injection facility in their models is due to aversion of hepatitis C infections (65).
A cost-effectiveness and cost-benefit study on an operational SCS in Vancouver, Insite, used data from 2008 to determine if the prevention of infections and deaths among people who inject drugs was of greater or lesser economic cost than the cost of operating the service (66). Mathematical modelling was used to estimate the number of new HIV infections and deaths averted each year, in conjunction with estimating the lifetime cost of a new HIV infection and the value of a life, to determine “…an identifiable portion of the societal benefits of Insite” (66). Authors used a figure of CAD 1.5 million as the annual operating cost of Insite for 2007; this included services such as addiction counselling, case management, primary healthcare, public health screening, addiction services, housing services, education, and peer counselling (66). Authors suggest that on average, Insite prevents 35 new cases of HIV per year, and three deaths, which provides a society benefit of more than CAD 6 million per year after accounting for program cost (66). Authors suggest that Insite “…is a good value for the resources that it consumes” (66).
vii. no increase in crime
A systematic review of six studies indicated that the implementation of supervised drug consumption facilities did not appear to contribute to increases in drug dealing or drug-related crime (51). Four of these studies examined the association between facility operation and crime in Sydney, Australia (51). One study describes the impact of Australia’s first Medically Supervised Injecting Centre (located in the Kings Cross locality of Sydney) on drug-related crime (51, 67). The SCS opened in 2001; data used for this study was collected at various time points between 1999 and 2002 (67). Four sources of data were used: police-recorded incidents in theft and robbery, daily “counts” of loitering made by an observer who walked a standardized route in Kings Cross, police-recorded incidents of possession or use of cocaine and narcotics, and key informant interviews conducted with community members who lived, frequented, and/or worked in Kings Cross (67). A time-series analysis was used to determine the impact of the SCS on crime and loitering (67). Analysis of the data failed to show increased robbery or theft offences in Kings Cross when the SCS opened; furthermore, authors found that in early 2001, a downward trend in both robbery and theft offences was observed (67). However, authors do note that there was evidence of increased crime prior to opening the SCS, though there was little to no sustained increase in loitering in front of or behind the SCS by people who use drugs and by people who sell drugs, and that any increases were not big enough to represent large increases in drug use or dealing, nor constitute a public nuisance problem (67).
In March of 2020, the Government of Alberta published the results of a review on supervised consumption services, and found with the exception of Edmonton, “…crime, as measured by police calls for service, generally increased in the immediate vicinity in contrast to areas beyond the immediate vicinity of the sites…” (68). Additionally, at the public consultations a variety of issues were raised, including “…increases in needle debris to increases in crime, and increases in overall social disorder since the sites opened” (68). Following the release of this report, a call for its retraction was issued by the Canadian Drug Policy Coalition, noting “[p]oor methodological quality, lack of transparency, and biased presentation of results” (69). A response to this report was published in January of 2021, noting that methodological limitations led to the poor assessment and measured change in crime, and thus the effects of SCS on crime (70).
Additionally, the findings of the Government of Alberta’s report stand in contrast to a report from Health Canada in 2008, which found that “…our analysis of police data for the DTE [Downtown Eastside of Vancouver] and surrounding areas showed no changes in rates of crime recorded by police. The majority of local residents, service providers, business owners and police did not notice any increases” (71).
viii. no increase in drug use or related risks
Belackova et al. note that this category encompasses “…injecting initiation, cutaneous [skin] infections, overdose rates, employment rates, cessation of injection drug use and community drug use patterns” (1). Skin infections related to intravenous injection include cellulitis, abscesses, myositis, and necrotising fasciitis (72). Factors associated with injection-related skin infections among individuals using a supervised injection facility (Insite) was examined using longitudinal data from a cohort study (73). The main outcome for the study was a current injection-related skin infection reported to a nurse that was visually confirmed (73). Over the two-year study period, the proportion of people who inject drugs reporting an injection-related skin infection did not increase; generally, it remained consistent, ranging from 6–10%, with a slight decline from baseline to first follow-up visit (73).
| Outcome types | Examples of SCS outcomes reported in the literature |
| Attracting or retaining high-risk, marginalized clients | Retaining individuals at increased risk of drug-related harms (74) Attracting high-risk people who inject drugs (56) Attracting marginalized people who inject drugs (18) |
| Management of overdose and decreased mortality | Access to drug-checking and/or identifying trends in drug supply (4, 46, 75–77) Overdose (including risks, prevention, reversal, symptoms, etc.) (12, 46, 58, 76–83) Mortality (due to overdose and other causes) (57, 59, 76, 80) Training in overdose response (47, 49, 76) Take-home naloxone programs (47–49) |
| Enhancement of safe injecting practices | High-risk behaviours (4, 12, 83) Educational intervention to improve injection practices (8) Promoting safer injection conditions (18, 60) |
| Change in public drug use and public amenities | Injecting in public (61, 83) Location of used injecting equipment (18, 61, 83) Public order (including public drug use) (18, 51) |
| Access to and/or uptake of treatment and other healthcare and social services | Access to and/or use of other health services (12, 76, 80, 84–86) Access to and/or use of drug dependent services (83), withdrawal management services (87), or detoxification services (63), or other addiction treatment (62) Access to and/or use of primary care services in general (18), or hepatitis C-related services (5, 6), or vaccination programs (7) |
| Prevention of transmission of blood-borne infections and associated economic benefits | Cost-effectiveness analysis, where benefits and cost reductions are mainly accrued from averting hepatitis C infections (65) Cost-effectiveness and cost-benefit analysis, where benefits and cost reduction are accrued from averting HIV infections 359 (66) |
| Change in crime rates | Drug trafficking or crime (18) Drug use or drug supply offences (67) Drug-related loitering, drug dealing or petty crime (71) |
| Change in drug use or related risks | Educational intervention for injection practices (8) Drug injecting practices (18) Cessation (62) |
| Other types of health and well-being outcomes | Social connectedness, community, or social capital (80, 84, 86, 88) Emotional support and stress reduction (84) Safety and/or security (78, 80, 84, 86, 88, 89) |
Table 1. Examples of SCS outcomes reported in the literature (outcome types adapted from Belackova et al. 2019) (1)
Factors that may impact local applicability
Several studies in this review include data that were collected and analyzed from clients of the first SCS, Insite, in 2003. As noted in the systematic review on evaluation methodologies, SCS outcomes are “highly skewed to two countries” – Canada and Australia, and one specific site in each country (1). Thus, broadening the scope of research will strengthen the evidence base (92). Study findings do not necessarily suggest that SCS in other locales will have the same results; the nature of the injection drug scene in a particular locale may have an effect on the harm reduction offerings at any given SCS, and the impact the SCS has on health outcomes. Additionally, operational guidance for SCS from the BCCSU notes that there are a variety of ways “…to plan, design, and implement a SCS” (22). Finally, this review should not be considered a comprehensive review on all structural, process, and outcome measures occurring at SCS in Canada and abroad; rather, it is a brief summary outlining some measures used in the literature to evaluate the impact of SCS.
What we did
We searched Medline (including Epub Ahead of Print, In-Process & Other Non-Indexed Citations) using terms (Supervised Injection Service* or Supervised Injection Site* or supervised drug consumption* or overdose prevention center* or overdose prevention centre* or supervised injection facilit* or drug consumption room* or drug consumption facilit* or safer drug use* service* or safe* injection facilit* or safe* injection site* or Overdose Prevention Site* or [Consumption adj3 Services*] or supervised consumption) in titles or abstracts. Searches were conducted on January 14, 2021 and results limited to English articles published from 2010 to present. Reference lists of identified articles were also searched. Google searches using above-mentioned terms were also conducted. The searches yielded 429 references from which 92 were included.
Reference list
- Belackova V, Salmon AM, Day CA, Ritter A, Shanahan M, Hedrich D, et al. Drug consumption rooms: A systematic review of evaluation methodologies. Drug & Alcohol Review. 2019;38(4):406–22.
- CATIE. Harm reduction in action: Supervised consumption services and overdose prevention sites. 2018. Available from: https://www.catie.ca/en/pif/fall-2018/harm-reduction-action-supervised-consumption-services-and-overdose-prevention-sites Accessed January 28, 2021.
- Government of British Columbia. Overdose prevention. 2021. Available from: https://www2.gov.bc.ca/gov/content/overdose/what-you-need-to-know/overdose-prevention Accessed: February 9, 2021.
- Karamouzian M, Dohoo C, Forsting S, McNeil R, Kerr T, Lysyshyn M. Evaluation of a fentanyl drug checking service for clients of a supervised injection facility, Vancouver, Canada. Harm Reduction Journal. 2018;15(1):46.
- Belackova V, Salmon AM, Schatz E, Jauncey M. Drug consumption rooms (DCRs) as a setting to address hepatitis C — Findings from an international online survey. Hepatology, Medicine and Policy. 2018;3(1):1–11.
- Lettner B. Hepatitis C treatment program at Moss Park Consumption and Treatment Service. 2019. Available from: https://www.catie.ca/en/pc/elements/mpcts Accessed February 1, 2021.
- Scherbaum N, Timm J, Richter F, Bonnet U, Bombeck J, Lajos S, et al. Outcome of a hepatitis B vaccination program for clients of a drug consumption facility. Journal of Clinical Virology. 2018;106:28–32.
- Mezaache S, Protopopescu C, Debrus M, Morel S, Mora M, Suzan-Monti M, et al. Changes in supervised drug-injecting practices following a community-based educational intervention: A longitudinal analysis. Drug & Alcohol Dependence. 2018;192:1–7.
- Government of Canada. Canada’s opioid crisis (fact sheet). 2019. Available from: https://www.canada.ca/content/dam/hc-sc/documents/services/publications/healthy-living/canada-opioid-crisis.pdf Accessed February 23, 2021.
- Government of Canada. Opioid- and stimulant-related harms in Canada. 2020. Available from: https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/#fn1-0-rf Accessed: March 1, 2021.
- Manson-Singer C, Allin S. Understanding the policy context and conditions necessary for the establishment of supervised consumption sites in Canada: A comparative analysis of Alberta and Manitoba. Health Reform Observer–Observatoire des Réformes de Santé. 2020;8(2).
- Magwood O, Salvalaggio G, Beder M, Kendall C, Kpade V, Daghmach W, et al. The effectiveness of substance use interventions for homeless and vulnerably housed persons: A systematic review of systematic reviews on supervised consumption facilities, managed alcohol programs, and pharmacological agents for opioid use disorder. PLoS ONE. 2020;15(1):e0227298.
- Government of Canada. General (continued): Regulations and Exemptions (continued): Exemption for medical purpose — Supervised consumption site. 2021. Available from: https://laws-lois.justice.gc.ca/eng/acts/c-38.8/page-12.html Accessed January 18, 2021.
- PHS Community Services Society. Insite. 2021. Available from: https://www.phs.ca/program/insite/ Accessed January 18, 2021.
- Government of Canada. Supervised consumption sites: Status of applications. 2021. Available from: https://www.canada.ca/en/health-canada/services/substance-use/supervised-consumption-sites/status-application.html Access January 18, 2020.
- National Harm Reduction Coalition. Training guide: Overview of supervised consumption services in the United States. 2020. Available from: https://harmreduction.org/issues/supervised-consumption-services/overview-united-states/ Accessed February 24, 2021.
- Government of Canada. Supervised consumption sites and services: Explained. 2020. Available from: https://www.canada.ca/en/health-canada/services/substance-use/supervised-consumption-sites/explained.html Accessed January 25, 2021.
- Potier C, Laprevote V, Dubois-Arber F, Cottencin O, Rolland B. Supervised injection services: What has been demonstrated? A systematic literature review. Drug & Alcohol Dependence. 2014;145:48–68.
- Lang K, Neil J, Wright J, Dell CA, Berenbaum S, El-Aneed A. Qualitative investigation of barriers to accessing care by people who inject drugs in Saskatoon, Canada: Perspectives of service providers. Substance Abuse Treatment, Prevention, and Policy. 2013;8(1):1–11.
- Wang L, Panagiotoglou D, Min JE, DeBeck K, Milloy M, Kerr T, et al. Inability to access health and social services associated with mental health among people who inject drugs in a Canadian setting. Drug and Alcohol Dependence. 2016;168:22–9.
- Miller-Lloyd L, Landry J, Macmadu A, Allard I, Waxman M. Barriers to healthcare for people who inject drugs: A survey at a syringe exchange program. Substance Use & Misuse. 2020;55(6):896–9.
- British Columbia Centre for Substance Abuse. Supervised consumption services: Operational guidance. 2017. Available from: https://www.bccsu.ca/wp-content/uploads/2017/07/BC-SCS-Operational-Guidance.pdf Accessed February 9, 2021.
- ACT Academy, NHS Improvement. Quality, service improvement and redesign tools: A model for measuring quality care. [Not dated]. Available from: https://improvement.nhs.uk/documents/2135/measuring-quality-care-model.pdf Accessed January 29, 2021.
- Donabedian A. Evaluating the quality of medical care. The Milbank Memorial Fund Quarterly. 1966;44(3):166–206.
- Donabedian A. The quality of care: How can it be assessed? Journal of the American Medical Association. 1988;260(12):1743–8.
- Cambridge University Press. Cambridge Dictionary: Meaning of data in English. 2021. Available from: https://dictionary.cambridge.org/dictionary/english/data Accessed January 19, 2021.
- Shah A. Using data for improvement. British Medical Journal. 2019;364(l189).
- Bryman A. Social research methods. 5th edition: Oxford University Press; 2016.
- Macalester College: Dewitt Wallace Library. Data module #1: What is research data? 2021. Available from: https://libguides.macalester.edu/c.php?g=527786&p=3608639#:~:text= Qualitative%20Data, compared%20on%20a%20numeric%20scale Accessed January 26, 2021.
- McGill Qualitative Health Research Group. Qualitative or quantitative research? [Not dated.] Available from: https://www.mcgill.ca/mqhrg/resources/what-difference-between-qualitative-and-quantitative-research Accessed January 25, 2021.
- Agency for Healthcare Research and Quality. Data sources for healthcare quality measures. 2018. Available from: https://www.ahrq.gov/talkingquality/measures/understand/index.html Accessed January 25, 2021.
- Canadian Institute for Health Information. Outcomes. 2021. Available from: https://www.cihi.ca/en/outcomes Accessed January 25, 2021.
- Dash S, Shakyawar SK, Sharma M, Kaushik S. Big data in healthcare: Management, analysis and future prospects. Journal of Big Data. 2019;6(1):1–25.
- Veillard J, Fekri O, Dhalla I, Klazinga N. Commentary no. 483: Measuring outcomes in the Canadian health sector: Driving better value from healthcare. 2015. Available from: https://www.cdhowe.org/sites/default/files/attachments/research_papers/mixed/Commentary_438.pdf Accessed January 25, 2021.
- Best M, Neuhauser D. Avedis Donabedian: Father of quality assurance and poet. BMJ Quality & Safety. 2004;13(6):472–3.
- Ayanian JZ, Markel H. Donabedian’s lasting framework for health care quality. The New England Journal of Medicine. 2016;375(3):205–7.
- Committee to Design a Strategy for Quality Review and Assurance in Medicare. Medicare: A strategy for quality assurance, Volume I. 1990. Available from: https://www.ncbi.nlm.nih.gov/books/NBK235462/pdf/Bookshelf_NBK235462.pdf Accessed February 1, 2021. Report No.: 0309042305.
- Health Quality Ontario. What is health quality. 2021. Available from: https://www.hqontario.ca/What-is-Health-Quality Accessed February 1, 2021.
- Mitra S, Rachlis B, Scheim A, Bardwell G, Rourke SB, Kerr T. Acceptability and design preferences of supervised injection services among people who inject drugs in a mid-sized Canadian City. Harm Reduction Journal. 2017;14(46):1–9.
- Watson TM, Strike C, Kolla G, Penn R, Jairam J, Hopkins S, et al. Design considerations for supervised consumption facilities (SCFs): Preferences for facilities where people can inject and smoke drugs. International Journal of Drug Policy. 2013;24(2):156–63.
- Speed KA, Gehring ND, Launier K, O’Brien D, Campbell S, Hyshka E. To what extent do supervised drug consumption services incorporate non-injection routes of administration? A systematic scoping review documenting existing facilities. Harm Reduction Journal. 2020;17(1):72.
- Montero-Moraga JM, Garrido-Albaina A, Barbaglia MG, Gotsens M, Aranega D, Espelt A, et al. Impact of 24-hour schedule of a drug consumption room on service use and number of non-fatal overdoses. A quasiexperimental study in Barcelona. International Journal of Drug Policy. 2020;81:102772.
- Government of Canada. Supervised consumption sites and services: Explained. 2020. Available from: https://www.canada.ca/en/health-canada/services/substance-use/supervised-consumption-sites/explained.html Accessed February 10, 2021.
- Xavier J, Rudzinski K, Guta A, Carusone SC, Strike C. Rules and eligibility criteria for supervised consumption services feasibility studies — A scoping review. International Journal of Drug Policy. 2020;88:103040.
- Schroers A. Drug checking: Monitoring the contents of new synthetic drugs. Journal of Drug Issues. 2002;32(2):635–46.
- Maghsoudi N, McDonald K, Stefan C, Beriault DR, Mason K, Barnaby L, et al. Evaluating networked drug checking services in Toronto, Ontario: Study protocol and rationale. Harm Reduction Journal. 2020;17(1):9.
- Dwyer R, Olsen A, Fowlie C, Gough C, van Beek I, Jauncey M, et al. An overview of take‐home naloxone programs in Australia. Drug and Alcohol Review. 2018;37(4):440–9.
- Lintzeris N, Monds LA, Bravo M, Read P, Harrod ME, Gilliver R, et al. Designing, implementing and evaluating the overdose response with take‐home naloxone model of care: An evaluation of client outcomes and perspectives. Drug and Alcohol Review. 2020;39(1):55–65.
- Wood W. Distributing take home naloxone via Sydney Medically Supervised Injecting Centre (MSIC) — Where to from here? 2015. Available from https://na.eventscloud.com/file_uploads/c0ef96bb7af3504eeeccda2ea89fa42a_1145tueWilliamWood.pdf Accessed February 25, 2021.
- Uniting. Uniting Medically Supervised Injecting Centre: Training workshops. 2021. Available from: https://www.uniting.org/community-impact/uniting-medically-supervised-injecting-centre–msic/training-opportunities Accessed February 25, 2021.
- Kennedy MC, Karamouzian M, Kerr T. Public health and public order outcomes associated with supervised drug consumption facilities: A systematic review. Current HIV/AIDS Reports. 2017;14(5):161–83.
- Semaan S, Fleming P, Worrell C, Stolp H, Baack B, Miller M. Potential role of safer injection facilities in reducing HIV and hepatitis C infections and overdose mortality in the United States. Drug & Alcohol Dependence. 2011;118(2-3):100–10.
- Kimber J, Dolan K, Van Beek I, Hedrich D, Zurhold H. Drug consumption facilities: An update since 2000. Drug and Alcohol Review. 2003;22(2):227–33.
- Kerr T, Kimber J, DeBeck K, Wood E. The role of safer injection facilities in the response to HIV/AIDS among injection drug users. Current HIV/AIDS Reports. 2007;4(4):158–64.
- Milloy MJ, Wood E. [Commentary] Emerging role of supervised injecting facilities in human immunodeficiency virus prevention. Addiction. 2009;104(4):620–1.
- Wood E, Tyndall MW, Li K, Lloyd-Smith E, Small W, Montaner JS, et al. Do supervised injecting facilities attract higher-risk injection drug users? American Journal of Preventive Medicine. 2005;29(2):126–30.
- Marshall BD, Milloy MJ, Wood E, Montaner JS, Kerr T. Reduction in overdose mortality after the opening of North America’s first medically supervised safer injecting facility: A retrospective population-based study. The Lancet. 2011;377(9775):1429–37.
- Scheim AI, Bouck Z, Tookey P, Hopkins S, Sniderman R, McLean E, et al. Supervised consumption service use and recent non-fatal overdose among people who inject drugs in Toronto, Canada. International Journal of Drug Policy. 2020;87:102993.
- Kennedy MC, Hayashi K, Milloy MJ, Wood E, Kerr T. Supervised injection facility use and all-cause mortality among people who inject drugs in Vancouver, Canada: A cohort study. PLoS Medicine. 2019;16(11):e1002964.
- Fast D, Small W, Wood E, Kerr T. The perspectives of injection drug users regarding safer injecting education delivered through a supervised injecting facility. Harm reduction journal. 2008;5(1):1–8.
- Salmon AM, Thein H-H, Kimber J, Kaldor JM, Maher L. Five years on: What are the community perceptions of drug-related public amenity following the establishment of the Sydney Medically Supervised Injecting Centre? International Journal of Drug Policy. 2007;18(1):46–53.
- DeBeck K, Kerr T, Bird L, Zhang R, Marsh D, Tyndall M, et al. Injection drug use cessation and use of North America’s first medically supervised safer injecting facility. Drug and Alcohol Dependence. 2011;113(2-3):172–6.
- Gaddis A, Kennedy MC, Nosova E, Milloy MJ, Hayashi K, Wood E, et al. Use of on-site detoxification services co-located with a supervised injection facility. Journal of Substance Abuse Treatment. 2017;82:1–6.
- PHS Community Services Society. Onsite. 2021. Available from: https://www.phs.ca/program/onsite/ Accessed February 4, 2021.
- Enns EA, Zaric GS, Strike CJ, Jairam JA, Kolla G, Bayoumi AM. Potential cost-effectiveness of supervised injection facilities in Toronto and Ottawa, Canada. Addiction. 2016;111(3):475–89.
- Andresen MA, Boyd N. A cost-benefit and cost-effectiveness analysis of Vancouver’s supervised injection facility. International Journal of Drug Policy. 2010;21(1):70–6.
- Freeman K, Jones CG, Weatherburn DJ, Rutter S, Spooner CJ, Donnelly N. The impact of the Sydney medically supervised injecting centre (MSIC) on crime. Drug and Alcohol Review. 2005;24(2):173–84.
- Government of Alberta. Impact: A socio-economic review of supervised consumption sites in Alberta. 2020. Available from: https://www.alberta.ca/release.cfm?xID=68744B5DE9A5D-D694-A553-44B691DDE7C56BF7 Accessed February 9, 2021.
- Canadian Drug Policy Coalition. Open letter: Calling on the Alberta Government to retract supervised consumption site report. 2020. Available from: https://www.drugpolicy.ca/open-letter-calling-on-the-alberta-government-to-retract-supervised-consumption-site-study/ Accessed February 25, 2021.
- Livingston JD. Supervised consumption sites and crime: Scrutinizing the methodological weaknesses and aberrant results of a government report in Alberta, Canada. Harm Reduction Journal. 2021;18(1):1–5.
- Health Canada. Vancouver’s INSITE service and other supervised injection sites: What has been learned from research? Final report of the Expert Advisory Committee on supervised injection site research. 2008. Available from: https://www.canada.ca/en/health-canada/corporate/about-health-canada/reports-publications/vancouver-insite-service-other-supervised-injection-sites-what-been-learned-research.html#con Accessed February 11, 2021.
- Delaney FT, Stanley E, Bolster F. The needle and the damage done: Musculoskeletal and vascular complications associated with injected drug use. Insights into Imaging. 2020;11(1):1–14.
- Lloyd-Smith E, Wood E, Zhang R, Tyndall MW, Montaner JS, Kerr T. Risk factors for developing a cutaneous injection-related infection among injection drug users: A cohort study. BMC Public Health. 2008;8(1):1–6.
- Kennedy MC, Klassen DC, Dong H, Milloy MS, Hayashi K, Kerr TH. Supervised injection facility utilization patterns: A prospective cohort study in Vancouver, Canada. American Journal of Preventive Medicine. 2019;57(3):330–7.
- Betsos A, Valleriani J, Boyd J, Bardwell G, Kerr T, McNeil R. “I couldn’t live with killing one of my friends or anybody”: A rapid ethnographic study of drug sellers’ use of drug checking. International Journal of Drug Policy. 2020;87:102845.
- Olding M, Ivsins A, Mayer S, Betsos A, Boyd J, Sutherland C, et al. A low-barrier and comprehensive community-based harm-reduction site in Vancouver, Canada. American Journal of Public Health. 2020;110(6):833–5.
- Notta D, Black B, Chu T, Joe R, Lysyshyn M. Changing risk and presentation of overdose associated with consumption of street drugs at a supervised injection site in Vancouver, Canada. Drug & Alcohol Dependence. 2019;196:46–50.
- Boyd J, Lavalley J, Czechaczek S, Mayer S, Kerr T, Maher L, et al. “Bed Bugs and Beyond”: An ethnographic analysis of North America’s first women-only supervised drug consumption site. International Journal of Drug Policy. 2020;78:102733.
- Kolla G, Kenny KS, Bannerman M, Boyce N, Chapman L, Dodd Z, et al. Help me fix: The provision of injection assistance at an unsanctioned overdose prevention site in Toronto, Canada. International Journal of Drug Policy. 2020;76:102617.
- Pauly B, Wallace B, Pagan F, Phillips J, Wilson M, Hobbs H, et al. Impact of overdose prevention sites during a public health emergency in Victoria, Canada. PLoS ONE. 2020;15(5):e0229208.
- Madah-Amiri D, Skulberg AK, Braarud AC, Dale O, Heyerdahl F, Lobmaier P, et al. Ambulance-attended opioid overdoses: An examination into overdose locations and the role of a safe injection facility. Substance Abuse. 2019;40(3):383–8.
- Kinshella MW, Gauthier T, Lysyshyn M. Rigidity, dyskinesia and other atypical overdose presentations observed at a supervised injection site, Vancouver, Canada. Harm Reduction Journal. 2018;15(1):64.
- Folch C, Lorente N, Majo X, Pares-Badell O, Roca X, Brugal T, et al. Drug consumption rooms in Catalonia: A comprehensive evaluation of social, health and harm reduction benefits. International Journal of Drug Policy. 2018;62:24–9.
- Kerman N, Manoni-Millar S, Cormier L, Cahill T, Sylvestre J. “It’s not just injecting drugs”: Supervised consumption sites and the social determinants of health. Drug & Alcohol Dependence. 2020;213:108078.
- McNeil R, Dilley LB, Guirguis-Younger M, Hwang SW, Small W. Impact of supervised drug consumption services on access to and engagement with care at a palliative and supportive care facility for people living with HIV/AIDS: a qualitative study. Journal of the International AIDS Society. 2014;17:18855.
- Foreman-Mackey A, Bayoumi AM, Miskovic M, Kolla G, Strike C. ‘It’s our safe sanctuary’: Experiences of using an unsanctioned overdose prevention site in Toronto, Ontario. International Journal of Drug Policy. 2019;73:135–40.
- Vipler S, Hayashi K, Milloy MJ, Wood E, Nosova E, Kerr T, et al. Use of withdrawal management services among people who use illicit drugs in Vancouver, Canada. Substance Abuse Treatment, Prevention, & Policy. 2018;13(1):27.
- Pijl E, Oosterbroek T, Motz T, Mason E, Hamilton K. Peer-assisted injection as a harm reduction measure in a supervised consumption service: A qualitative study of client experiences. Harm Reduction Journal. 2021;18(1):5.
- Boyd J, Collins AB, Mayer S, Maher L, Kerr T, McNeil R. Gendered violence and overdose prevention sites: A rapid ethnographic study during an overdose epidemic in Vancouver, Canada. Addiction. 2018;113(12):2261–70.
- Oudshoorn A, Sangster Bouck M, McCann M, Zendo S, Berman H, Banninga J, et al. A critical narrative inquiry to understand the impacts of an overdose prevention site on the lives of site users. Harm Reduction Journal. 2021;18(1):6.
- Kennedy MC, Hayashi K, Milloy MJ, Boyd J, Wood E, Kerr T. Supervised injection facility use and exposure to violence among a cohort of people who inject drugs: A gender-based analysis. International Journal of Drug Policy. 2020;78:102692. May T, Holloway K, Bennett T. The need to broaden and strengthen the evidence base for supervised consumption sites. Addiction. 2019;114(12):2117–8.
- May T, Holloway K, Bennett T. The need to broaden and strengthen the evidence base for supervised consumption sites. Addiction. 2019;114(12):2117–8.
Suggested citation
Rapid Response Service. A review of structural, process, and outcome measures for supervised consumption services. Toronto, ON: The Ontario HIV Treatment Network; March 2021.
Prepared by
Danielle Giliauskas and David Gogolishvili
Photo credit